HOME > Publication & Reports > Annual Report 2016 > Hospital East
Department of Plastic and Reconstructive Surgery
Ryuichi Hayashi, Takuya Higashino, Azusa Oshima, Shuchi Azuma, Yu Hokazono
Introduction
The Department of Plastic and Reconstructive Surgery has mainly focused on surgical reconstruction following cancer ablation. In our institution, reconstructive procedures using free flap transfer with microvascular anastomosis are the most important operations. In addition, several methods such as tissue transfer with pedicled flaps, local flaps, and skin grafting are used for reconstructive surgery. The objectives of reconstructive surgery are not only the morphological reconstruction, but also the restoration of postoperative functions after ablative surgery. The quality of life (QOL) of patients can be improved with functional and morphological reconstruction.
Our team and what we do
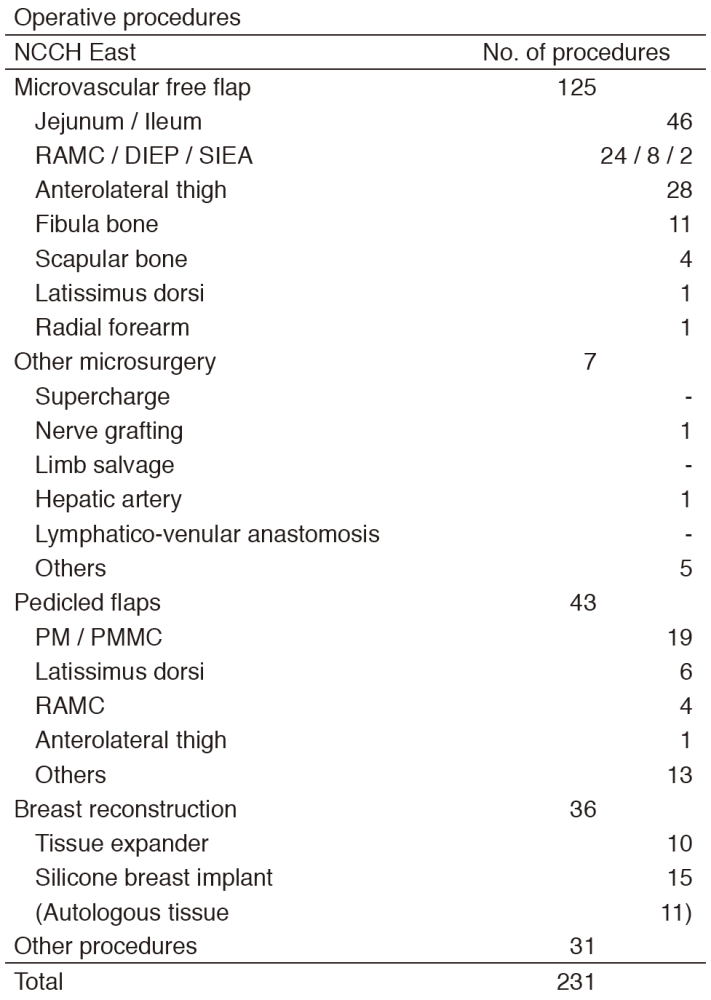
Five plastic surgeons cover reconstructive operations both in the National Cancer Center Hospital (NCCH) East in Kashiwa and the NCCH in Tokyo, in which residents are trained in both hospitals. The reconstructive surgeries are performed in cooperation with surgeons of other departments within the hospital, such as the Department of Head and Neck Surgery, Breast Surgery, Esophageal Surgery, Thoracic Surgery, Colorectal Surgery, and Urology (Table 1). In the NCCH East, Head and Neck reconstruction is the most frequently performed operation accounting for about 60% of the reconstructive surgeries. In the Head and Neck region, a free jejunal transfer and anterolateral thigh flap transfer are the most frequently used procedures (Table 2). A weekly conference is held with doctors of the Department of Head and Neck surgery, Radiation Oncology, and Head and Neck Medical Oncology. Breast reconstruction using autologous tissue transfer was employed in 2005, since then, patients'needs for breast reconstruction is increasing. Furthermore, lymphatico-venular anastomosis as a surgical treatment for lymphedema of the extremities was introduced in 2013.
Table 1. Number of patients
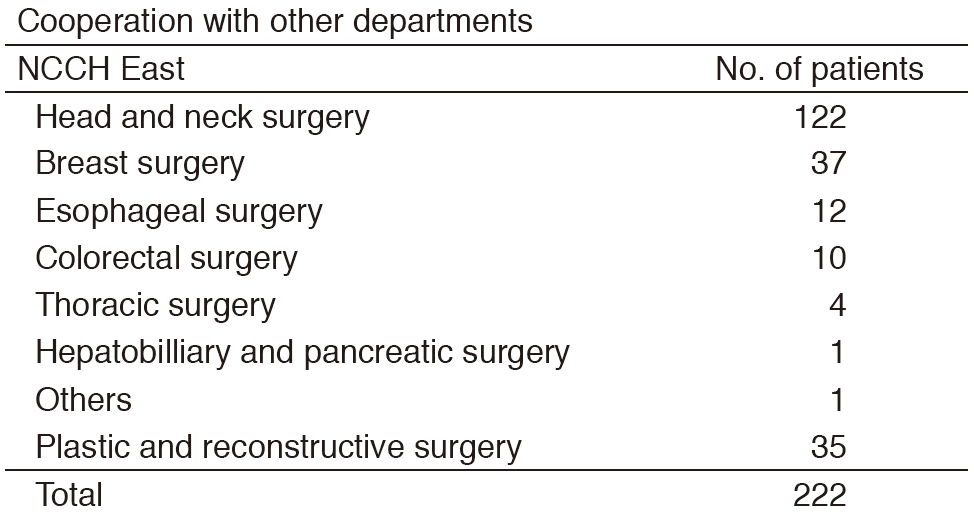
Table 2. Type of procedures
Research activities
Plastic and reconstructive surgery has focused on the following four aspects in the surgical treatment of cancer for the purpose of contributing to the improvement of the QOL of patients.
1)Obtaining good functional recovery
2)Reduction of postoperative complications
3)Achieving less donor site morbidity
4)Treatment of postoperative complications after cancer ablation.
With the objective of addressing these four aspects establishing a standard for reconstructive surgery and developing new techniques of reconstructive surgery are the most important aims of our studies. Multi-institutional analysis of postoperative complication and swallowing function after total pharyngo-laryngo-esophagectomy and reconstruction with a free jejunal transfer was performed continuously. This study was supported by a Grant in-Aid for Cancer Research. The aim of the study is to clarify the relationship between surgical procedures and postoperative complication and function.
In 2015, we also started to take an active part in a new multi-institutional analysis of risk factors for functional outcome after tongue reconstruction.
Education
We accept a lot of young plastic surgeons from all over Japan as residents and train them to become reconstructive surgeons. We also train them to become future opinion leaders in the field of reconstructive surgery.
Future prospects
The promotion of multi-institutional studies concerning reconstructive surgery will provide our patients with high-precision medical services based on evidence.
List of papers published in 2016
Journal
1.Kimata Y, Matsumoto H, Sugiyama N, Onoda S, Sakuraba M. Lessons Learned from Unfavorable Microsurgical Head and Neck Reconstruction: Japan National Cancer Center Hospital and Okayama University Hospital. Clin Plast Surg, 43:729-737, 2016
2.Fujiki M, Miyamoto S, Zenda S, Sakuraba M. Longitudinal and long-term effects of radiotherapy on swallowing function after tongue reconstruction. J Laryngol Otol, 130:865-872, 2016
3.Higashino T, Sakuraba M, Oshima A, Fujiki M, Miyamoto S. Single venous anastomosis versus dual venous anastomoses in free anterolateral thigh flap transfer: A cohort study. J Plast Reconstr Aesthet Surg, 69:1313-1315, 2016
4.Fujiki M, Sakuraba M, Miyamoto S, Hayashi R. Predictive factors of dysphagia after lateral and superior oropharyngeal reconstruction with free flap transfer. J Surg Oncol, 113:240-243, 2016
5.Fujiki M, Miyamoto S, Kobayashi E, Sakuraba M, Chuman H. Early detection of local recurrence after soft tissue sarcoma resection and flap reconstruction. Int Orthop, 40:1975-1980, 2016
6.Miyamoto S, Arikawa M, Fujiki M, Kawai A, Kobayashi E, Sakuraba M. The Superior Rectal Artery as a Recipient Vessel for Free Flap Transfer After Partial Sacrectomy in Patients With Chordoma. Ann Plast Surg, 76:315-317, 2016
7.Ooishi M, Motegi A, Kawashima M, Arahira S, Zenda S, Nakamura N, Ariji T, Tokumaru S, Sakuraba M, Tahara M, Hayashi R, Akimoto T. Patterns of failure after postoperative intensity-modulated radiotherapy for locally advanced and recurrent head and neck cancer. Jpn J Clin Oncol, 46:919-927, 2016
8.Enokida T, Fujii S, Kuno H, Mukaigawa T, Tahara M, Sakuraba M, Hayashi R. Combined salivary duct carcinoma and squamous cell carcinoma suspected of carcinoma ex pleomorphic adenoma. Pathol Int, 66:460-465, 2016