HOME > Publication & Reports > Annual Report 2016 > Hospital
Department of Plastic and Reconstructive Surgery
Shimpei Miyamoto, Masaki Arikawa, Yu Kagaya, Kensuke Tashiro
Introduction
The Department of Plastic and Reconstructive Surgery has mainly focused on surgical reconstruction after cancer ablation. In our institution, reconstructive procedures using free flap transfer with microvascular anastomosis are the most important operations. In addition, several methods such as tissue transfer with pedicled flaps, local flaps, skin grafts, and so forth, are used for reconstructive surgery. The objectives of reconstructive surgery are not only morphological reconstruction, but also restoration of postoperative functions after ablative surgery. The quality of life (QOL) of the patient can be improved by functional and morphological reconstruction.
Table 1. Reconstructive procedures
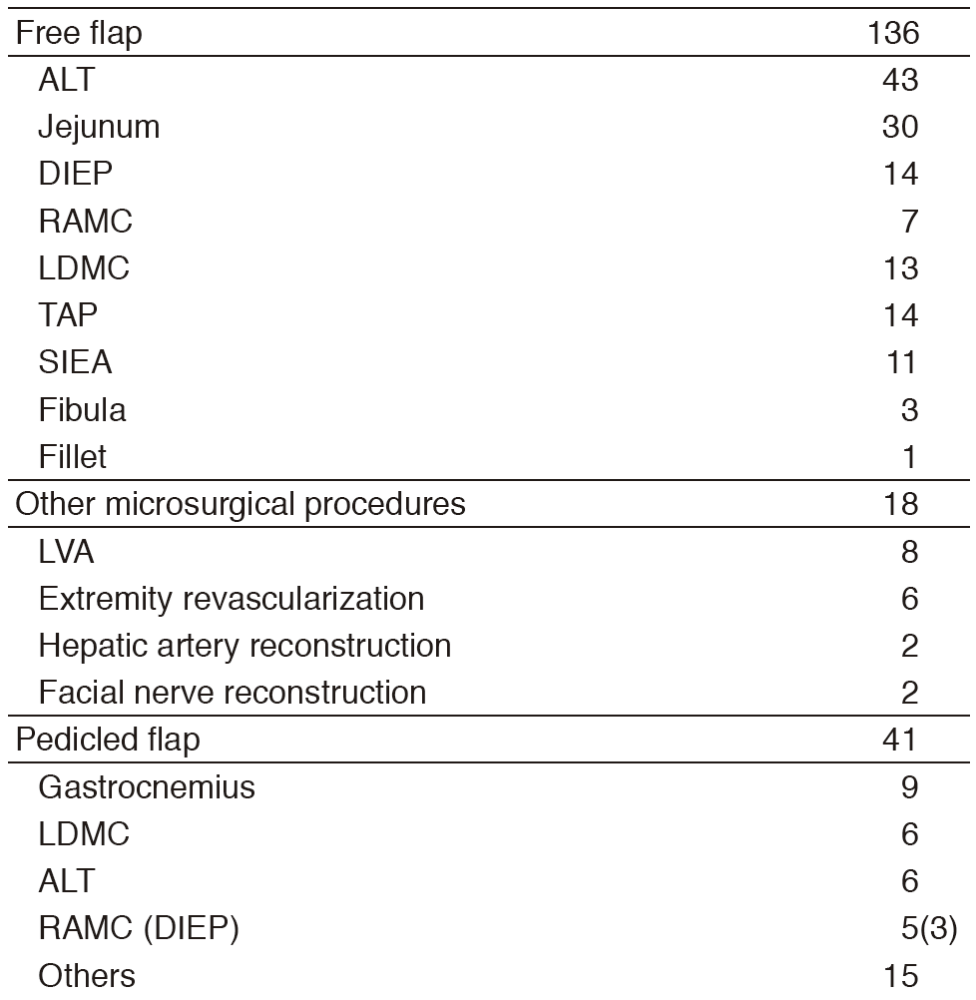
Routine activities
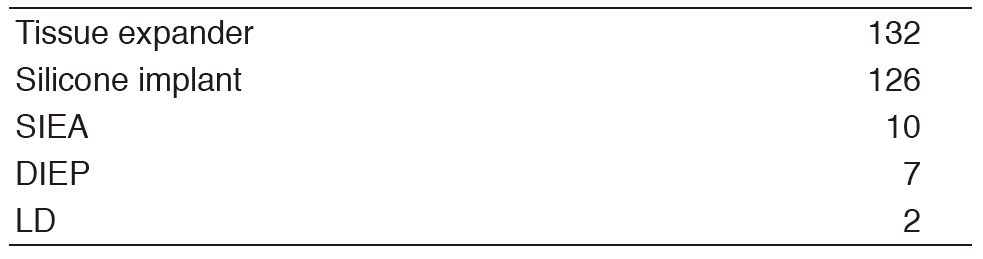
Three plastic surgeons cover reconstructive operations. Every week, five to ten reconstructive operations are performed. These reconstructive surgeries are performed in cooperation with surgeons from other departments of the hospital, such as Head and Neck Oncology, Breast Surgery, Musculoskeletal Oncology and Rehabilitaion, Esophageal Surgery, and Dermatologic Oncology. The number of patients who receive immediate breast reconstruction is increasing. Most patients undergo breast reconstruction with a silicone implant. Limb reconstruction after limb preservation surgery has increased.
Table 2. Breast reconstruction

Research activities
Multi-institutional analysis of postoperative functions after microvascular tongue reconstruction is ongoing. Also, laboratory research on flow-through flaps using a rat model is ongoing.
List of papers published in 2016
Journal
1.Fujiki M, Miyamoto S, Zenda S, Sakuraba M. Longitudinal and long-term effects of radiotherapy on swallowing function after tongue reconstruction. J Laryngol Otol, 130:865-872, 2016
2.Fujiki M, Sakuraba M, Miyamoto S, Hayashi R. Predictive factors of dysphagia after lateral and superior oropharyngeal reconstruction with free flap transfer. J Surg Oncol, 113:240-243, 2016
3.Fujiki M, Miyamoto S, Kobayashi E, Sakuraba M, Chuman H. Early detection of local recurrence after soft tissue sarcoma resection and flap reconstruction. Int Orthop, 40:1975-1980, 2016
4.Miyamoto S, Arikawa M, Fujiki M, Kawai A, Kobayashi E, Sakuraba M. The Superior Rectal Artery as a Recipient Vessel for Free Flap Transfer After Partial Sacrectomy in Patients With Chordoma. Ann Plast Surg, 76:315-317, 2016
5.Miyamoto S, Fujiki M, Sakisaka M, Kawai A. Combined Use of the Latissimus Dorsi Musculocutaneous Flap and the Anterolateral Thigh Flap to Reconstruct an Extensive Shoulder Defect in an NF-1 Patient. Plast Reconstr Surg Glob Open, 4:e670, 2016
6.Miyamoto S, Fujiki M, Setsu N, Kawai A. Simultaneous reconstruction of the bone and vessels for complex femoral defect. World J Surg Oncol, 14:291, 2016
7.Tashiro K, Fujiki M, Arikawa M, Kagaya Y, Miyamoto S. Free Flap Salvage after Recurrent Venous Thrombosis by Means of Large-Scale Treatment with Medical Leeches. Plast Reconstr Surg Glob Open, 4:e1157, 2016
8.Miyamoto S, Sakuraba M, Nagamatsu S, Fujiki M, Fukunaga Y, Hayashi R. Combined use of anterolateral thigh flap and pharyngeal flap for reconstruction of extensive soft-palate defects. Microsurgery, 36:291-296, 2016
9.Fujiki M, Sakuraba M, Miyamoto S, Nagamatsu S, Hayashi R. A "no-touch-technique" in mandibular reconstruction with reconstruction plate and free flap transfer. Microsurgery, 36:115-120, 2016