HOME > Publication & Reports > Annual Report 2016 > Hospital
Department of Breast Surgery
Takayuki Kinoshita, Shin Takayama, Sota Asaga, Kenjiro Jimbo, Sho Shiino, Eriko Iwamoto, Toshiaki Kurihara
Introduction
The Department of Breast Surgery deals with treatment of breast cancer thorough surgeries, as well as diagnosis of breast diseases and assessment of lymph nodes in the axillary and clavicular regions which are suspected of harboring metastases. The trend of surgical procedure has been changing year by year. Although breast partial resection (Bp) accounted for 36% of the total surgeries in our department in 2016, Bp is on the decline in recent years. One of the reasons is the increasing needs of immediate reconstruction surgeries. In our hospital, since 2010, immediate breast reconstruction became one of the choices for patients in whom breast preservation were cosmetically difficult, and a total of 155 immediate breast reconstructions were performed in 2016, comprising 21% of all cases. One hundred and thirty-one out of 155 were tissue expander (TE), and direct implant (DIM). Fourteen were autologous reconstruction (12 DIEP; deep inferior epigastric perforator flap, and two LD; latissimus dorsi muscle flap). We perform these reconstruction surgeries in cooperation with plastic surgeon depending on the patients'needs. In addition, the new, less invasive technique, radiofrequency abrasion (RFA), is another reason. In 2016, 54 RFA were performed. The number of cases in immediate breast reconstructions and RFAs has gradually increased year by year to match the increasing needs of patients. Sentinel lymph node (SLN) biopsies (SLNB) were performed in 83% of the cases. Following SLNB, the axillary lymph node dissection (ALND) could be avoided when the SLNB was negative. One-step nucleic acid amplification (OSNA) assay, that quantitatively measures CK19 mRNA detects sentinel lymph node metastases even in molecular levels in conjunction with this assay and conventional microscopic method, we began to be able to evaluate the SLN more precisely. Further, by comparing the OSNA results with that of conventional histological diagnosis, we try to search the possibility of omitting axillary lymph node dissection by using two methods. Thus, to meet the diverse needs of breast cancer patients, we are striving continuously.
Routine activities
Our department is comprised of five staff surgeons, one chief resident, and three or four rotating residents. From 7:20 every morning, all the staff and the residents perform patient rounds together. Journal clubs and research conferences are scheduled for every Tuesday morning after rounds. Weekly conferences are held on Monday from 18:00 to 19:30, and on Wednesday from 17:00 to 18:00 for shared discussions with surgeons, medical oncologists, radiologists, and radiology and sonography technicians. The diagnostic images of pre-operative patients are reviewed and compared to pathological reports in every postoperative patient. A breast pathology/imaging conference is held on the second Wednesday of each month from 19:00 to 20:00 to discuss problems with diagnostic imaging, and with pathologically interesting cases. A conference about studies, institutional treatment guidelines, and recent topics regarding breast cancer is held on the last Wednesday of each month by a multidisciplinary team. Treatment Guidelines for primary and metastatic breast cancer have been updated regularly through multidisciplinary discussion since 2003.
Surgery
We perform surgeries from Monday to Friday, and 15 to 18 cases of breast cancer are performed regularly within each week.
Table 1 shows a total number of patients with primary breast cancer (including breast primary sarcoma) and other breast disease. The type and number of operative procedures are shown in Table 2. The rate of mastectomy was 57% (415/736), including 155 cases of immediate reconstruction. SLNB was performed in 578 patients, and 501 patients were spared from ALND in 2016.
Research activities and Clinical trials
1.Radiofrequency ablation therapy for early breast cancer as local therapy (RAFAELO study)
Trial of image-guided radiofrequency ablation (non-surgical therapy) has accomplished for early-stage breast carcinomas of less than 1.0 cm in a diameter (Phase I/II study; Kinoshita et al.). After years of the trial, the indication has just been expanded up to 1.5 cm in a diameter and this technique is certified as an advanced medical treatment by the Ministry of Health, Labour and Welfare. Our secondary goals are to determine the size, configuration, and pathological features of the acute RFA treatment of breast cancers, and we have conducted clinical studies to evaluate the oncologic safety of RFA in terms of local recurrence.
2.Intensive vs. standard post-operative surveillance in high risk breast cancer patients (JCOG1204, INSPIRE Trial)
This is a multi-center randomized phase III trial that started in 2012. This clinical trial is to prove the hypothesis that postoperative intensive follow-up for patients with breast cancer is good for a standard follow-up.
3.Denosumab adjuvant treatment (D-CARE)
This phase III multi-center, randomized, double blind, placebo controlled study has continued, designed to compare the treatment effect of denosumab with that of a placebo on prolonging bone metastasis-free survival in subjects with early-stage breast cancer at high risk of disease recurrence.
4.Scalp-cooling device during chemotherapy
A feasibility study to test the use of a scalp-cooling device that breast cancer patients will wear while undergoing chemotherapy treatment has started and continued in order to slow or halt hair loss during chemotherapy.
5.Postoperative Therapy with Endocrine and TS-1 (POTENT study)
This multi-center randomized trial continued from 2012. This study compares invasive disease-free survival in patients with or without TS-1 administration together with adjuvant endocrine therapy in hormone positive and HER2 negative high recurrence risk patients.
6.Registration Data-base System of the breast cancer patient who had carried out the lymph node metastasis diagnosis by the OSNAR method (LynoLog Data-base)
The aim of this study is to accumulate the administrative data on cases with the OSNA method in a common database, LynoLog Database, and to evaluate the clinical significance of intraoperative SLN metastases detected by OSNA.
7.Olaparib as Adjuvant Treatment in Patients With Germline BRCA Mutated High Risk HER2 Negative Primary Breast Cancer (OlympiA)
A randomized, double-blind, parallel group, placebo-controlled multi-centre phase III study started in 2014. The aim of study is to assess the efficacy and safety of olaparib versus placebo as adjuvant treatment in patients with germline BRCA1/2 mutations, and high risk HER2 negative primary breast cancer who have completed definitive local treatment and neoadjuvant or adjuvant chemotherapy.
8.Hair Loss Prevention System with chemotherapy-induced alopecia in breast cancer patients in Japan (HOPE)
This study is a multi-center controlled trial of PAX-15. This clinical trial is to prove the prevention effect of a scalp-cooling device that prevents hair loss during chemotherapy.
Table 1. Number of patients
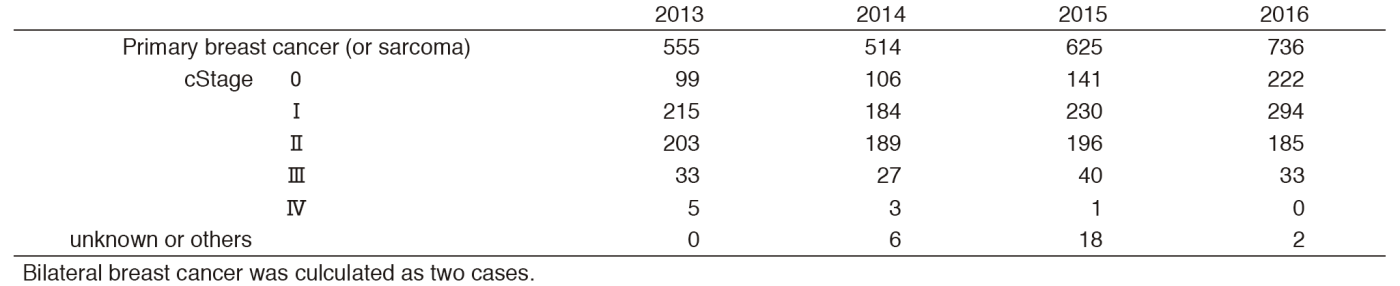
Table 2-1. Type of procedures (breast surgery)
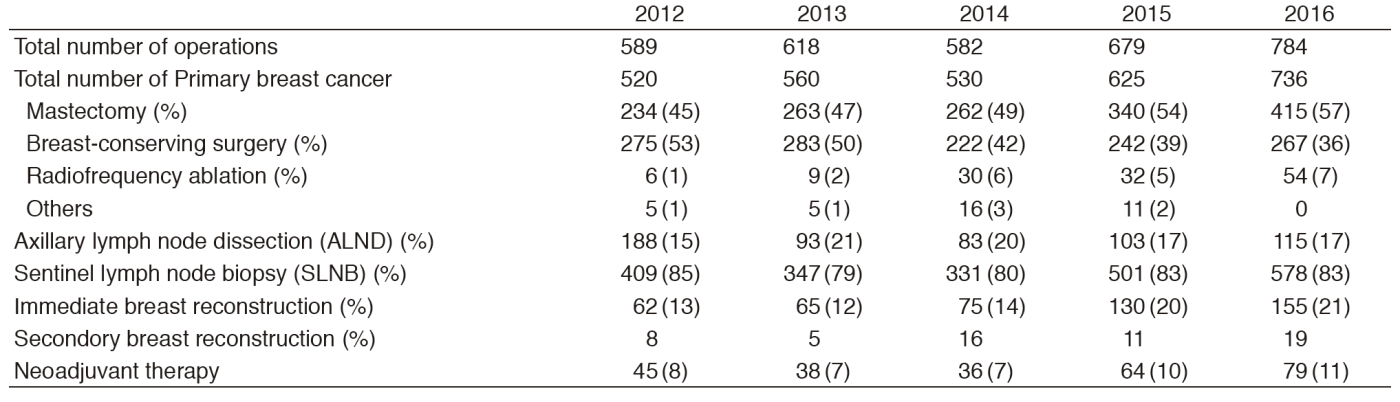
Table 2-2. Type of procedures (reconstruction surgery, 2016.1-12)


Table 3. Survival (2003-2008)


List of papers published in 2016
Journal
1.Anan K, Fukui N, Kinoshita T, Iwamoto T, Niikura N, Kawai M, Hayashi N, Tsugawa K, Aogi K, Ishida T, Masuoka H, Masuda S, Iijima K, Nakamura S, Tokuda Y. Comprehensive prognostic report of the Japanese Breast Cancer Society Registry in 2005. Breast Cancer, 23:50-61, 2016
2.Iwamoto T, Fukui N, Kinoshita T, Anan K, Niikura N, Kawai M, Hayashi N, Tsugawa K, Aogi K, Ishida T, Masuoka H, Masuda S, Iijima K, Nakamura S, Tokuda Y. Comprehensive prognostic report of the Japanese Breast Cancer Society registry in 2006. Breast Cancer, 23:62-72, 2016
3.Niikura N, Tomotaki A, Miyata H, Iwamoto T, Kawai M, Anan K, Hayashi N, Aogi K, Ishida T, Masuoka H, Iijima K, Masuda S, Tsugawa K, Kinoshita T, Nakamura S, Tokuda Y. Changes in tumor expression of HER2 and hormone receptors status after neoadjuvant chemotherapy in 21 755 patients from the Japanese breast cancer registry. Ann Oncol, 27:480-487, 2016
4.Masai K, Kinoshita T, Jimbo K, Asaga S, Hojo T. Clinicopathological features of breast angiosarcoma. Breast Cancer, 23:718-723, 2016
5.Sato Y, Kinoshita T, Suzuki J, Jimbo K, Asaga S, Hojo T, Yoshida M, Tsuda H. Preoperatively diagnosed ductal carcinoma in situ: risk prediction of invasion and effects on axillary management. Breast Cancer, 23:761-770, 2016
6.Tamura N, Tsuda H, Yoshida M, Hojo T, Akashi-Tanaka S, Kinoshita T, Sugihara K. Clinicopathological predictive factors for ipsilateral and contralateral events following initial surgery to treat ductal carcinoma in situ. Breast Cancer, 23:510-518, 2016
7.Kinoshita T, Fukui N, Anan K, Iwamoto T, Niikura N, Kawai M, Hayashi N, Tsugawa K, Aogi K, Ishida T, Masuoka H, Masuda S, Iijima K, Nakamura S, Tokuda Y. Comprehensive prognostic report of the Japanese Breast Cancer Society Registry in 2004. Breast Cancer, 23:39-49, 2016
8.Kawai M, Tomotaki A, Miyata H, Iwamoto T, Niikura N, Anan K, Hayashi N, Aogi K, Ishida T, Masuoka H, Iijima K, Masuda S, Tsugawa K, Kinoshita T, Nakamura S, Tokuda Y. Body mass index and survival after diagnosis of invasive breast cancer: a study based on the Japanese National Clinical Database-Breast Cancer Registry. Cancer Med, 5:1328-1340, 2016
9.Iwamoto T, Kumamaru H, Miyata H, Tomotaki A, Niikura N, Kawai M, Anan K, Hayashi N, Masuda S, Tsugawa K, Aogi K, Ishida T, Masuoka H, Iijima K, Matsuoka J, Doihara H, Kinoshita T, Nakamura S, Tokuda Y. Distinct breast cancer characteristics between screen- and self-detected breast cancers recorded in the Japanese Breast Cancer Registry. Breast Cancer Res Treat, 156:485-494, 2016
10.Shiino S, Kinoshita T, Yoshida M, Jimbo K, Asaga S, Takayama S, Tsuda H. Prognostic Impact of Discordance in Hormone Receptor Status Between Primary and Recurrent Sites in Patients With Recurrent Breast Cancer. Clin Breast Cancer, 16:e133-140, 2016
11.Kataoka A, Iwamoto T, Tokunaga E, Tomotaki A, Kumamaru H, Miyata H, Niikura N, Kawai M, Anan K, Hayashi N, Masuda S, Tsugawa K, Aogi K, Ishida T, Masuoka H, Iijima K, Kinoshita T, Nakamura S, Tokuda Y. Young adult breast cancer patients have a poor prognosis independent of prognostic clinicopathological factors: a study from the Japanese Breast Cancer Registry. Breast Cancer Res Treat, 160:163-172, 2016
Book
1.Kinoshita T (ed), Non-surgical ablation therapy for early-stage breast cancer, Springer International Publishing AG, 2016