HOME > Publication & Reports > Annual Report 2016 > Hospital
Department of Gastric Surgery
Hitoshi Katai, Takeo Fukagawa, Shinji Morita, Hisataka Fujiwara, Takeyuki Wada, Hiroshi Moro, Yuya Satoh, Toshiro Nishida
Introduction
The Department of Gastric Surgery treats not only gastric adenocarcinoma but also sarcomas of gastric origin, such as malignant lymphomas or gastrointestinal stromal tumors (GISTs). Principally, we treat tumors of the esophagogastric junction.
Routine activities
Our department includes five staff surgeons, two chief residents and three or four rotating residents at any given time. Nine to eleven patients are operated upon every week. Patients with stage I disease are followed-up without adjuvant chemotherapy. Adjuvant S-1 chemotherapy is used for patients with stage II and III disease. Adjuvant XELOX chemotherapy is applied for stage IIIC disease. Neoadjuvant chemotherapy is frequently used for patients with locally advanced tumors.
Patients with a superficial well-differentiated adenocarcinoma lesion are treated with endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD). Some undergo subsequent surgery based on the histological findings of the resected specimen. Every Tuesday from 6:15 to 7:00 P.M., a clinical conference is held for surgeons, a medical oncologist, and endoscopists. All patients with gastric malignancies in the ward or on the waiting list for admission are briefly reviewed and those whose treatment is controversial are discussed in detail. Every Friday between 7:15 and 8:30 A.M., another clinical conference is held, in which surgeons and endoscopists present all candidates for surgical and endoscopic treatment for the following week, and the treatment strategy for each case is discussed in detail. On the third Wednesday of every month, between 6:00 and 7:00, pathological conference is held, in which endoscopists and pathologists discuss. These conferences are held in English whenever a foreign guest doctor is present.
We consider the education of foreign surgeons to be an important function. In 2016, more than 20 surgeons from various countries visited this department for one week to eight months to learn about the management of gastric cancer patients, especially surgical techniques for lymph node dissection and postoperative care. All staff surgeons have sufficient experience in teaching in English.
Research activities
Several translational studies are being carried out in cooperation with the National Cancer Center Research Institute. Genomic scanning in gastric cancer is being carried out. DNA methylation as a gastric cancer metastasis risk factor has been investigated. A mini-chip assay of peritoneal washings for prediction of gastric cancer recurrence is being developed. Research on the detection of small amounts of cancer cells in peripheral blood and bone marrow of gastric cancer patients is being carried out.
Clinical trials
Our department has been playing a central role in conducting multi-institutional clinical trials. H. Katai is a representative of the Gastric Cancer Surgical Study Group of the Japan Clinical Oncology Group (JCOG). Patients with gastric cancer are, when eligible, invited to participate in one of the ongoing clinical trials mentioned below. The JCOG 0501 phase III trial to evaluate the effect of neo-adjuvant (S-1 and CDDP) and adjuvant chemotherapy (S-1) for large type III and type IV tumors has been completed for accrual. The JCOG 1001, which is designed to evaluate the significance of bursectomy for advanced cancer, was carried out and the results were reported. The JCOG 0912 phase III trial to prove the non-inferiority of laparoscopic gastrectomy over its open counterpart for patients with clinical stage IA and IB gastric cancer has been completed for accrual. The phase II trial to prove the feasibility of laparoscopic total and proximal gastrectomy for stage IA and IB gastric cancer (JCOG 1401) has also been completed for accrual.
The JCOG 1104 phase III trial to evaluate the optimal period of adjuvant S-1 chemotherapy for pathological stage II gastric cancer patients who underwent D2 gastrectomy is ongoing. The JCOG1301C, a randomized phase II study of systemic chemotherapy with and without trastuzumab followed by surgery in HER2 positive advanced gastric or esophagogastric junction adenocarcinoma with extensive lymph node metastasis is ongoing.
The JCOG 1507 phase III trial to confirm S-1 adjuvant chemotherapy for pathological stage II/III vulnerable elderly gastric cancer patients, and the JCOG 1509 phase III trial to evaluate the efficacy of neoadjuvant chemotherapy with S-1 plus oxalliplatin followed by D2 gastrectomy with adjuvant S-1 in locally advanced gastric cancer were just started.
Table 1. Number of Patients

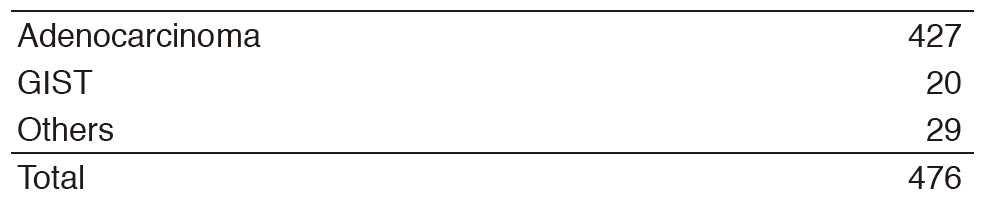
Table 2. Operative morbidity and mortality after gastrectomy
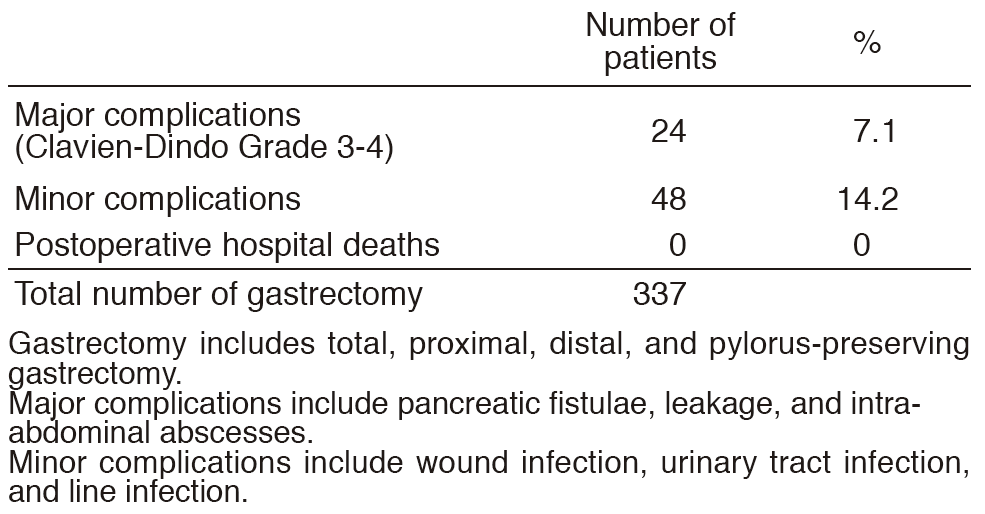
Table 3. Operative Procedures
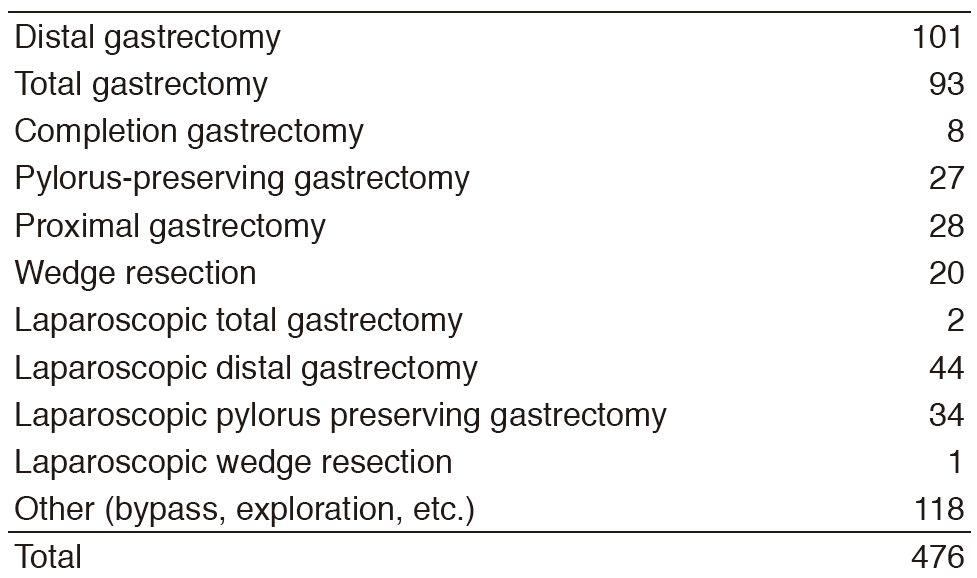
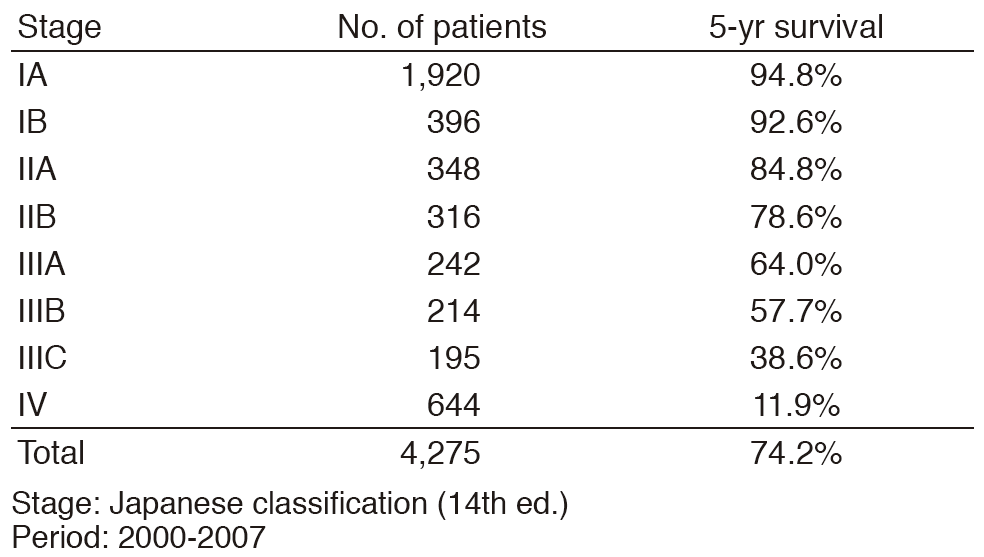
Table 4. Overall Survival Rates
Education
Education of surgical operations has been introduced for chief and rotating residents throughout the perioperative management of approximately 500 gastric cancer patients.
Future prospects
D2 gastrectomy is considered the standard surgical treatment for advanced gastric cancer but multi-modality treatments combined with surgery will further improve survival rates. There are several surgical options for early gastric cancer depending on the risk of nodal metastasis. The efficacy of laparoscopic surgery for early gastric cancer is being assessed. Moreover, robotic surgery is introduced as advanced medical care services and the safety and effectiveness have currently been evaluated. These procedures will require good quality control achieved through supervision and training by experienced surgeons in high volume centers.
List of papers published in 2016
Journal
1.Rokutan H, Hosoda F, Hama N, Nakamura H, Totoki Y, Furukawa E, Arakawa E, Ohashi S, Urushidate T, Satoh H, Shimizu H, Igarashi K, Yachida S, Katai H, Taniguchi H, Fukayama M, Shibata T. Comprehensive mutation profiling of mucinous gastric carcinoma. J Pathol, 240:137-148, 2016
2.Takizawa K, Ono H, Yamamoto Y, Katai H, Hori S, Yano T, Umegaki E, Sasaki S, Iizuka T, Kawagoe K, Shimoda T, Muto M, Sasako M. Incidence of lymph node metastasis in intramucosal gastric cancer measuring 30 mm or less, with ulceration; mixed, predominantly differentiated-type histology; and no lymphovascular invasion: a multicenter retrospective study. Gastric Cancer, 19:1144-1148, 2016
3.Kataoka K, Katai H, Mizusawa J, Katayama H, Nakamura K, Morita S, Yoshikawa T, Ito S, Kinoshita T, Fukagawa T, Sasako M. Non-Randomized Confirmatory Trial of Laparoscopy-Assisted Total Gastrectomy and Proximal Gastrectomy with Nodal Dissection for Clinical Stage I Gastric Cancer: Japan Clinical Oncology Group Study JCOG1401. J Gastric Cancer, 16:93-97, 2016
4.Kamata T, Sunami K, Yoshida A, Shiraishi K, Furuta K, Shimada Y, Katai H, Watanabe S, Asamura H, Kohno T, Tsuta K. Frequent BRAF or EGFR mutations in ciliated muconodular papillary tumors of the lung. J Thorac Oncol, 11:261-265, 2016
5.Zong L, Hattori N, Yoda Y, Yamashita S, Takeshima H, Takahashi T, Maeda M, Katai H, Nanjo S, Ando T, Seto Y, Ushijima T. Establishment of a DNA methylation marker to evaluate cancer cell fraction in gastric cancer. Gastric Cancer, 19:361-369, 2016
6.Morita S, Fukagawa T, Fujiwara H, Katai H. Questionnaire survey regarding the current status of super-extended lymph node dissection in Japan. World J Gastrointest Oncol, 8:707-714, 2016
7.Morita S, Fukagawa T, Fujiwara H, Katai H. The clinical significance of para-aortic nodal dissection for advanced gastric cancer. Eur J Surg Oncol, 42:1448-1454, 2016
8.Ohashi M, Morita S, Fukagawa T, Wada T, Kushima R, Onaya H, Katai H. Evaluation of 64-Channel Contrast-Enhanced Multi-detector Row Computed Tomography for Preoperative N Staging in cT2-4 Gastric Carcinoma. World J Surg, 40:165-171, 2016
9.Honma Y, Yamada Y, Terazawa T, Takashima A, Iwasa S, Kato K, Hamaguchi T, Shimada Y, Ohashi M, Morita S, Fukagawa T, Machida N, Katai H. Feasibility of neoadjuvant S-1 and oxaliplatin followed by surgery for resectable advanced gastric adenocarcinoma. Surg Today, 46:1076-1082, 2016
10.Sekiguchi M, Oda I, Taniguchi H, Suzuki H, Morita S, Fukagawa T, Sekine S, Kushima R, Katai H. Risk stratification and predictive risk-scoring model for lymph node metastasis in early gastric cancer. J Gastroenterol, 51:961-970, 2016