HOME > Publication & Reports > Annual Report 2016 > Hospital
Department of Gynecology
Tomoyasu Kato, Shunichi Ikeda, Mitsuya Ishikawa, Takashi Uehara, Hanako Shimizu
Introduction
The Department of Gynecology deals with tumors originating from the female genital and reproductive organs. Surgery is the main treatment modality for most gynecologic cancers, but multidisciplinary treatments consisting of radiotherapy and chemotherapy are routinely considered in close cooperation with therapeutic radiation oncologists and medical oncologists. The incidences of three common gynecologic cancers, that is, cervical, endometrial, and ovarian cancer, are now on the rise in Japan.
Our team and what we do
* Nerve-sparing radical hysterectomy
* Para aortic lymphadenectomy
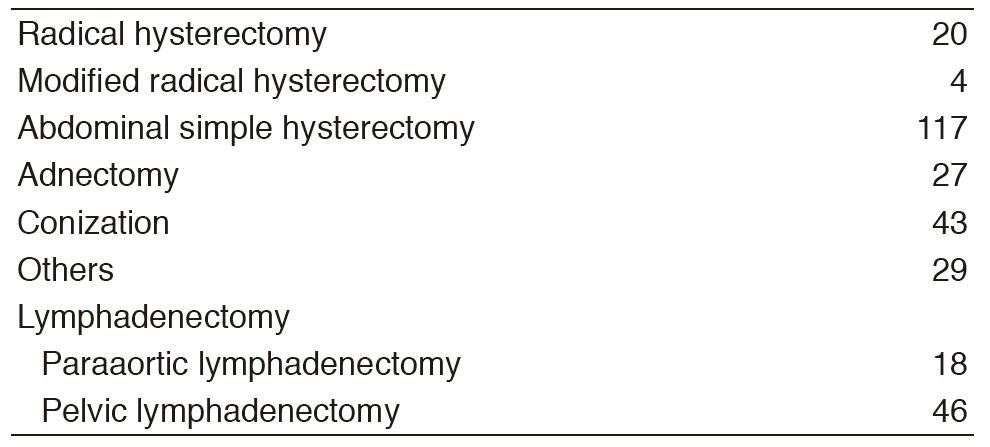
The number of operations in 2016 was 315 cases. That of radical hysterectomy was 20, which was slightly fewer than previous years. The paraaortic lymph node dissection was often the 18 cases.
We have been continuing to practice performing the extended operation reliably.
Research activities
1)Ascites cell block system: To investigate the diagnostic utility of the ascites cell block system (CB), 48 patients with diagnosed carcinomatous peritonitis were reviewed retrospectively between 2010 and 2014. Ascites CB sections were stained with hematoxylin and eosin (HE), and immunohistochemistry. Of the 48 patients, 32 had peritoneal cancer or ovarian cancer, three had endometrial cancers, four had breast cancers, six had digestive system malignancies, and three had peritoneal mesotheliomas. A total of seven patients (14.5%) were different between clinical diagnosis (symptom, image, and tumor marker) and the diagnosis by CB. A specific immunochemistry panel was helpful for the estimation of primary lesion, especially in the diagnosis of the digestive system origin.
2)In collaboration with the Department of Radiation Oncology, we showed the reduction of intestinal disturbance by using postoperative intensity modulated radiation therapy (IMRT) for patients with cervical cancer. It led to the creation of the protocol of concurrent chemoradiation therapy (CCRT) using IMRT for high-risk group of JCOG 1402 cervical cancer postoperative surgery.
Clinical trials
1)A non-randomized confirmatory trial of modified radical hysterectomy for patients with FIGO Stage Ib1 (< 2 cm) uterine cervical cancer (JCOG1101) is ongoing as planned.
2) A non-randomized verification study regarding selection of fertility-sparing surgery for patients with epithelial ovarian cancer (JCOG1203) is ongoing as planned.
3)A randomized phase II/III trial conventional paclitaxel and carboplatin versus dose-dense paclitaxel and carboplatin in stage IVB, recurrent, or persistent cervical carcinoma (JCOG 1311) has amended.
4)A randomized phase III trial to confirm survival effects of para-aortic lymphadnectomy for patients with endometrial cancer (JCOG1412) has started.
5)A non-randomized confirmatory trial of postoperative CCRT using IMRT for patients with curatively resected high-risk uterine cervical cancer has been submitted.
Table 1. Number of patients
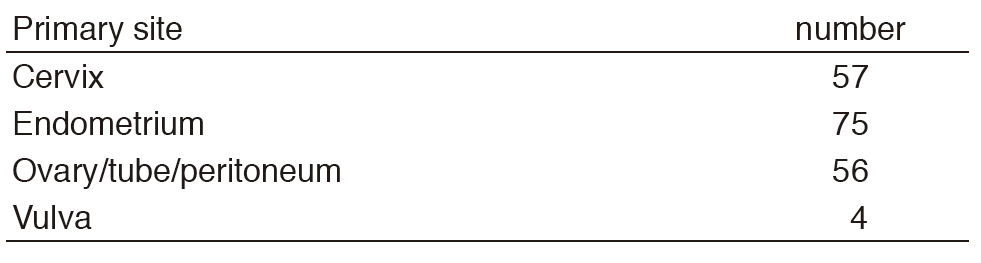
Table 2. Type of procedures
Education
* Chief resident doctor1
* Resident doctor6
Future prospects
We will promote to appeal extended surgery to be performed safely as we have been doing so far. In addition, we are striving for the control of peritoneal dissemination of ovarian cancer in collaboration with the National Cancer Center Research Institute (NCCRI).
List of papers published in 2016
Journal
1.Miyoshi Y, Yorifuji T, Horikawa R, Takahashi I, Nagasaki K, Ishiguro H, Fujiwara I, Ito J, Oba M, Kawamoto H, Fujisaki H, Kato M, Shimizu C, Kato T, Matsumoto K, Sago H, Takimoto T, Okada H, Suzuki N, Yokoya S, Ogata T, Ozono K. Gonadal function, fertility, and reproductive medicine in childhood and adolescent cancer patients: a national survey of Japanese pediatric endocrinologists. Clin Pediatr Endocrinol, 25:45-57, 2016
2.Bun S, Yunokawa M, Ebata T, Shimomura A, Shimoi T, Kodaira M, Yonemori K, Shimizu C, Fujiwara Y, Kato T, Makino Y, Hayashi Y, Tamura K. Feasibility of dose-dense paclitaxel/carboplatin therapy in elderly patients with ovarian, fallopian tube, or peritoneal cancer. Cancer Chemother Pharmacol, 78:745-752, 2016
3.Ebata T, Yunokawa M, Bun S, Shimomura A, Shimoi T, Kodaira M, Yonemori K, Shimizu C, Fujiwara Y, Kato T, Tamura K. Dose-dense paclitaxel plus carboplatin as neoadjuvant chemotherapy for advanced ovarian, fallopian tube, or primary peritoneal carcinomas. Cancer Chemother Pharmacol, 78:1283-1288, 2016
4.Kyo S, Kato T, Nakayama K. Current concepts and practical techniques of nerve-sparing laparoscopic radical hysterectomy. Eur J Obstet Gynecol Reprod Biol, 207:80-88, 2016
5.Murakami N, Kato T, Miyamoto Y, Nakamura S, Wakita A, Okamoto H, Tsuchida K, Kashihara T, Kobayashi K, Harada K, Kitaguchi M, Sekii S, Takahashi K, Umezawa R, Inaba K, Ito Y, Igaki H, Itami J. Salvage High-dose-rate Interstitial Brachytherapy for Pelvic Recurrent Cervical Carcinoma After Hysterectomy. Anticancer Res, 36:2413-2421, 2016
6.Murakami N, Kobayashi K, Kato T, Nakamura S, Wakita A, Okamoto H, Shima S, Tsuchida K, Kashihara T, Harada K, Takahashi K, Umezawa R, Inaba K, Ito Y, Igaki H, Itami J. The role of interstitial brachytherapy in the management of primary radiation therapy for uterine cervical cancer. J Contemp Brachytherapy, 8:391-398, 2016
7.Murakami N, Norihisa Y, Isohashi F, Murofushi K, Ariga T, Kato T, Inaba K, Okamoto H, Ito Y, Toita T, Itami J. Proposed definition of the vaginal cuff and paracolpium clinical target volume in postoperative uterine cervical cancer. Pract Radiat Oncol, 6:5-11, 2016
8.Takahashi K, Yoshida H, Watanabe R, Ishikawa M, Ikeda SI, Kato T. Metastasis of extra-ampullary duodenal adenocarcinoma to the uterine cervix. Malays J Pathol, 38:45-48, 2016