Annual Report 2017
Department of Breast Surgery
Takashi Hojo, Chisako Yamauchi, Tatsuya Onishi
Introduction
We treat patients with operable malignant mammary glands. Diagnosis of breast disease, surgical treatment and follow-up for breast cancer patients are our main professional practice. The Department of Breast Surgery consists of three staff surgeons and one resident, and is committed to providing the latest, most comprehensive breast treatments for our patients. The multidisciplinary approach to the diagnosis and treatment of cancer is carried out under cooperation among related specialists: surgeons, radiologists, plastic surgeons, pathologists, medical oncologists, specialized nurses, and technicians.
Our department mainly focuses on "minimally invasive surgery" and performs a thorough investigation for an oncologically safe approach, less morbidity and good cosmesis. For example, although sentinel lymph node (SLN) biopsy has already been established as the standard care for clinical node negative patients, omitting axillary lymph node dissection (ALND) for positive SLNs with micro- or macrometastasis has started in clinical practice as an expanded indication. On the other hand, preoperative systemic therapy provides the opportunity for a curative operation or breast-conserving surgery to avoid mastectomy. Moreover, we can provide breast reconstructive surgery in collaboration with the Department of Plastic and Reconstructive Surgery. These procedures will contribute to a better quality of life for patients with breast cancer.
Our team and what we do
For the regular activities of our department, a daily morning routine round is scheduled for inpatients by all staff and residents. Moreover, our weekly preoperative diagnostic imaging conference on breast cancer is conducted on Monday evenings to discuss the surgical treatment planning for each patient. A clinical conference to decide on courses of treatment by multidisciplinary breast care team members is held twice a month. A monthly pathological conference on breast cancer is also conducted on the last Friday of each month. At those conferences, individual cases are presented to a team of highly trained cancer specialists, including radiologists, breast surgeons, pathologists, radiation oncologists, and medical oncologists. Indeed, our multidisciplinary team approach to breast cancer treatment sets the quality of care we provide for our patients well apart from the norm.
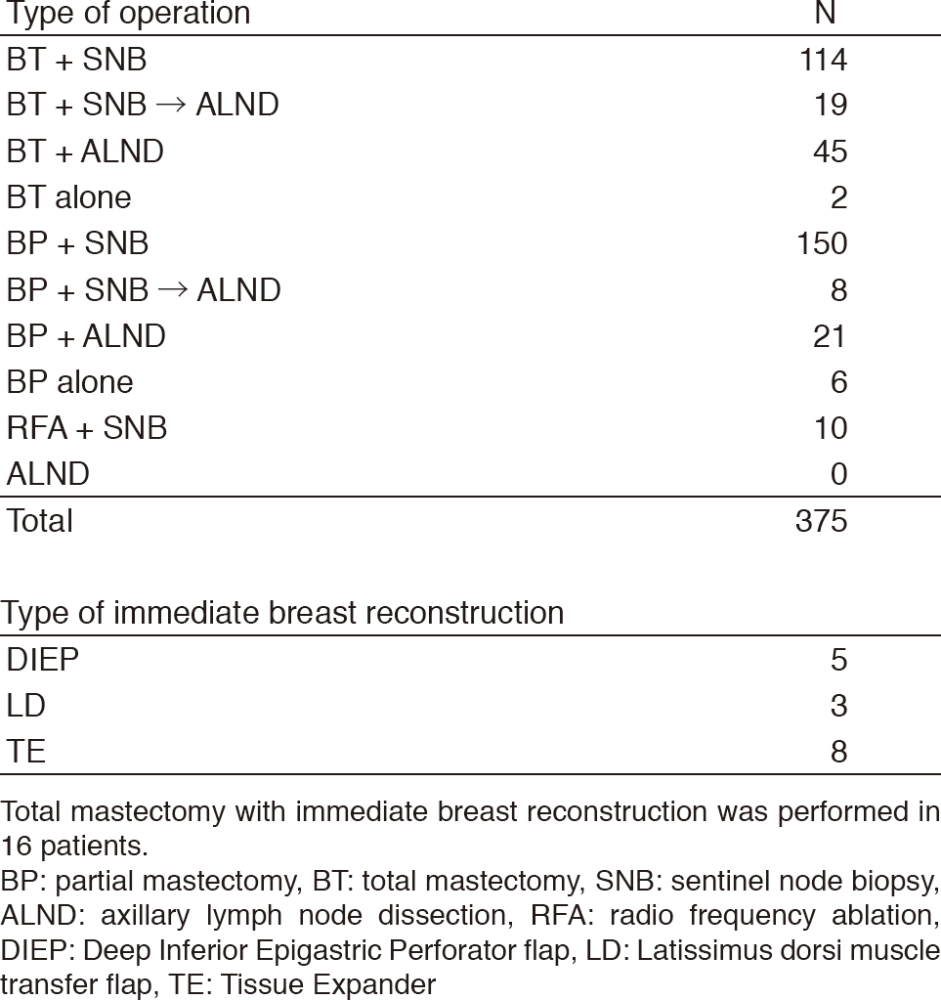
Changes in the annual number of patients with breast cancer who underwent surgery are shown in Table 1. A total of 375 patients with primary breast cancer and 52 patients with recurrence or other breast disease were operated on. Sixteen immediate breast reconstruction surgeries were included. Of the patients with primary breast cancer, 65 (17%) underwent primary systemic therapy. The types and number of operative procedures performed in 2017 are shown in Table 2. The rate of breast-conserving surgeries (including two radiofrequency ablation alone cases) was 52% (195/375). Sentinel node biopsy was performed in 301 patients, and 27 patients were spared from ALND.
Table 1. Number of primary breast cancer patients operated on during 2008-2017

Table 2. Type of operative procedures performed in 2017 for primary breast cancer
Research activities
1) Examination of the effectiveness between anthracycline regimen and anthracycline + taxan regimen for the ER-positive HER2-negative breast cancer. A retrospective search using National Clinical Database of a prospectively maintained was performed. Patients with less than four metastasis to axillary lymph node did not have the additional effectiveness of the taxane. We concluded that only the breast cancer patients with more than three axillary lymph node metastasis had the additional effectiveness of the taxane.
2) We perform the study to measure the hardness of the arms of the patients of lymphedema using a sensor of the hardness. In this study, we examine the relations of an evaluation of the hardness and the evaluation of lymphedema.
Clinical trials
1) Radiofrequency ablation (RFA) using a Cool-tip electrode system (RAFAELO study): A phase II study on RFA without resection was performed for T=<1.5 cm, N0 breast cancer patients with no extensive intraductal components using a Cool-tip electrode system. This study is certified as an advanced medical treatment by the Ministry of Health, Labour and Welfare.
2) Effectiveness of primary tumor resection for metastatic breast cancer (JCOG 1017): In this multicenter clinical trial, the primary tumor resection plus systemic therapy arm is compared to the systemic therapy alone arm in metastatic breast cancer.
3) Intensive vs. standard post-operative surveillance in high-risk breast cancer patients (JCOG1204, INSPIRE Trial): This is a multi-center randomized phase III trial which started in 2012. This clinical trial is to confirm the superiority of intensive follow-up to standard follow-up in terms of overall survival in high-risk breast cancer patients.
Education
Targets of our education are to raise knowledge about breast disease, and to improve operative techniques.
Future prospects
We want to deliver the appropriate postoperative follow-up care, which has been a longtime concern in breast cancer medical care. And we aim at more operative development with a minimally invasive surgery.