Annual Report 2017
Department of Urology
Hiroyuki Fujimoto, Motokiyo Komiyama, Yoshiyuki Matsui, Tomohiko Hara, Yasuo Shinoda, Aiko Maejima, Yuuta Toyoshima
Introduction
In the Department of Urology, all urogenital malignant diseases, including kidney cancer, urothelial cancer, prostate cancer, testicular germ cell tumors, and retroperitoneal sarcomas, are the subjects of diagnosis and treatment with comprehensive approaches, including radical surgery, irradiation, and chemotherapy.
Our team and what we do
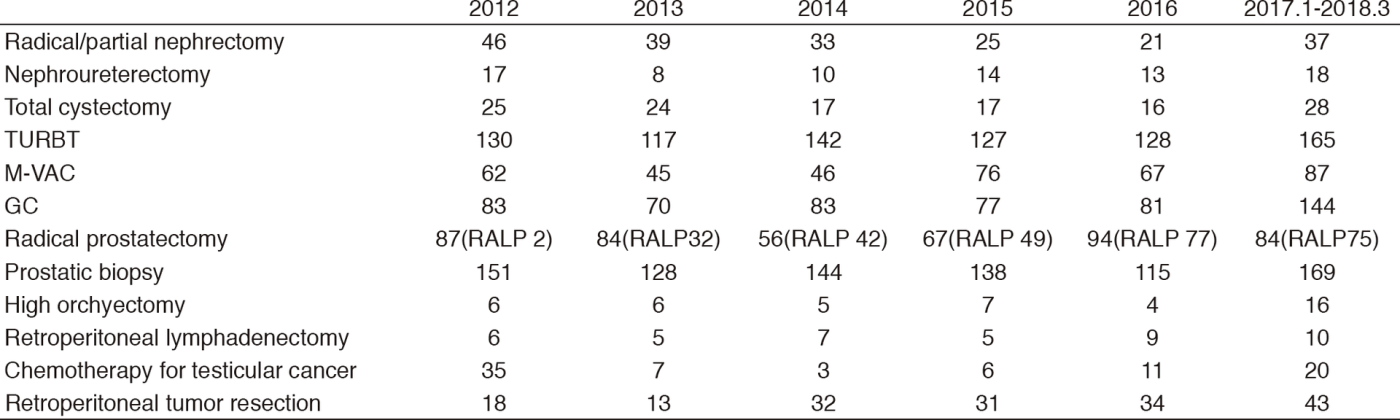
The urology team consists of six staff physicians, one chief-resident, and one resident. In addition, with the participation of a radiation oncologist, multi-disciplinary treatments for advanced diseases including renal cancer, urothelial cancer, hormone-refractory prostate cancer and metastatic germ cell tumors, are performed. Every morning clinical rounds start at 7:30 a.m., and a weekly conference to discuss inpatient management is held on Monday evenings. Patient statistics by major treatment were summarized in Table 1.
Major urological malignant diseases are treated according to the following strategies:
1) Renal cell carcinoma: M0, partial or radical nephrectomy; M1: chemotherapy with target drugs with TKI or mTOR with or without palliative nephrectomy. A selected small size (less than 3 cm) tumor: cryothearpy
2) Bladder cancer. Carcinoma in situ: BCG instillation therapy. Ta, T1, transurethral resection of bladder cancer (TURBT), often combined with preoperative or postoperative BCG instillation. T2-T4, radical cystectomy with neoadjuvant chemotherapy by an M-VAC/GC regimen. N+, systemic chemotherapy, radiation; sometimes urinary diversion alone. M+, chemotherapy with an M-VAC or GC regimen
3) Prostate cancer. Organ-confined disease, active surveillance, robotic-assisted or open radical prostatectomy, irradiation, or endocrine therapy. Specimen-confined disease, extended radical prostatectomy without neoadjuvant endocrine therapy, radiation therapy with endocrine therapy, or endocrine therapy alone. For high risk prostate cancer, extended pelvic lymph node dissection by robotic was performed. M1 disease, endocrine therapy and palliative radiation if necessary. For castration refractory disease, docetaxel or cabazitaxel chemotherapy is indicated.
4) Testicular germ cell tumor (GCT): Stage I, careful observation regardless of a pathological element. Stage II or higher, EP (etoposide + CDDP) or BEP (BLM + etoposide + CDDP) chemotherapy as the first line. In nonseminomatous cases, a salvage operation is performed after induction chemotherapy. In seminoma cases, careful observation rather than surgery is selected.
Research activities
We are constantly seeking ways to improve the treatment for malignant urological tumors.
1) Urothelial cancer: The effectiveness of a phase III study to confirm the efficacy of pirarubicin in the prevention of bladder recurrence after radical nephroureterectomy for upper tract urothelial carcinoma (JCOG1403) is ongoing. For metastatic disease, a weekly CBDCA + PTX regimen has been indicated.
2) Prostate cancer: A phase II study to evaluate the efficacy of robotic assisted laparoscopic radical prostatectomy for T1c-T3a prostate cancer is no longer recruiting. A new robotic operative method to achieve a complete surgical margin (extended radical prostatectomy) has been developed, and its efficacy in patients with specimen-confined disease has been evaluated without neoadjuvant endocrine therapy. This method was introduced in robotic assisted laparoscopic radical prostatectomy with extended lymph node dissection.
3) Testicular germ cell tumors (GCTs) : Advanced and/or refractory cases: A so-called "desperate operation", which was designed for patients whose tumor markers do not normalize after induction chemotherapy, has been shown to be both efficacious and clinically significant. For CDDP-refractory germ cell tumors, a second line TIP/TIN regimen has completed enrollment.
Clinical trials
We are actively involved in the following mainly ongoing protocol studies:
1) A phase III study: A single early intravesical instillation of pirarubicin in the prevention of bladder recurrence after radical nephroureterectomy for upper tract urothelial carcinoma (JCOG1403)
2) A phase III study: Anti PD-L1 antibody (ATEZOLIZUMAB/ MPDL3280A) for muscle invasive bladder cancer
3) A phase II study: Robotic assisted laparoscopic prostatectomy for intermediate or high risk prostate cancer
4) A phase II study: ICG navigated pelvic LN dissection for robotic assisted laparoscopic prostatectomy
List of papers published in January 2017 - March 2018
Journal
1. Hara T, Fujimoto H, Kondo T, Shinohara N, Obara W, Kimura G, Kume H, Nonomura N, Hongo F, Sugiyama T, Kanayama HO, Takahashi M, Fukumori T, Eto M. Active heavy cigarette smoking is associated with poor survival in Japanese patients with advanced renal cell carcinoma: sub-analysis of the multi-institutional national database of the Japanese Urological Association. Jpn J Clin Oncol, 47:1162-1169, 2017
2. Makise N, Yoshida A, Komiyama M, Nakatani F, Yonemori K, Kawai A, Fukayama M, Hiraoka N. Dedifferentiated Liposarcoma With Epithelioid/Epithelial Features. Am J Surg Pathol, 41:1523-1531, 2017
3. Suzuki H, Inoue Y, Fujimoto H, Yonese J, Tanabe K, Fukasawa S, Inoue T, Saito S, Ueno M, Otaka A. Diagnostic performance and safety of NMK36 (trans-1-amino-3-[18F] fluorocyclobutanecarboxylic acid)-PET/CT in primary prostate pancer: multicenter Phase IIb clinical trial. Jpn J Clin Oncol, 47:283, 2017
4. Inokuchi J, Eto M, Hara T, Fujimoto H, Nishiyama H, Miyazaki J, Kikuchi E, Hinotsu S, Koie T, Ohyama C. Impact of lymph node dissection on clinical outcomes during nephroureterectomy in patients with clinically node-negative upper urinary tract urothelial cancer: subanalysis of a multi-institutional nationwide case series of the Japanese Urological Association. Jpn J Clin Oncol, 47:652-659, 2017
5. Ohara K, Arai E, Takahashi Y, Ito N, Shibuya A, Tsuta K, Kushima R, Tsuda H, Ojima H, Fujimoto H, Watanabe SI, Katai H, Kinoshita T, Shibata T, Kohno T, Kanai Y. Genes involved in development and differentiation are commonly methylated in cancers derived from multiple organs: a single-institutional methylome analysis using 1007 tissue specimens. Carcinogenesis, 38:241-251, 2017
6. Inokuchi J, Kuroiwa K, Kakehi Y, Sugimoto M, Tanigawa T, Fujimoto H, Gotoh M, Masumori N, Ogawa O, Eto M, Ohyama C, Yamaguchi A, Matsuyama H, Ichikawa T, Asano T, Mizusawa J, Eba J, Naito S. Role of lymph node dissection during radical nephroureterectomy for upper urinary tract urothelial cancer: multi-institutional large retrospective study JCOG1110A. World J Urol, 35:1737-1744, 2017
7. Asano N, Yoshida A, Mitani S, Kobayashi E, Shiotani B, Komiyama M, Fujimoto H, Chuman H, Morioka H, Matsumoto M, Nakamura M, Kubo T, Kato M, Kohno T, Kawai A, Kondo T, Ichikawa H. Frequent amplification of receptor tyrosine kinase genes in welldifferentiated/ dedifferentiated liposarcoma. Oncotarget, 8:12941-12952, 2017