Annual Report 2018
Department of Esophageal Surgery
Hiroyuki Daiko, Takeo Fujita, Hisashi Fujiwara
Introduction
The Department of Esophageal Surgery deals with neoplasms arising from the esophagus. The surgical management of esophageal cancer has been the main clinical and research activity of this department. In particular, our department is striving to establish minimally invasive surgery that consists of neoadjuvant treatment followed by minimally invasive esophagectomy. Our department is conducting a study to define the role of surgery in the multimodal approach to the treatment of esophageal cancer, and is aiming for thoraco-laparoscopic esophagectomy, which consists of thoracoscopic esophagectomy and laparoscopic reconstruction, to become a standard surgical procedure.
The Team and What We Do
Our team performed 155 thoracic esophagectomies in 2018. Additionally, we dealt with 21 cases of cervical esophageal cancer (11 total laryngopharynx esophagectomies, ten larynx preserved esophagectomies). We also focused on postoperative care after surgery. We held patient support multidisciplinary classroom lessons six times in 2018. On the other hand, regarding academic activities, we attended and made speeches at seven domestic academic conferences and one international academic conference in 2018.
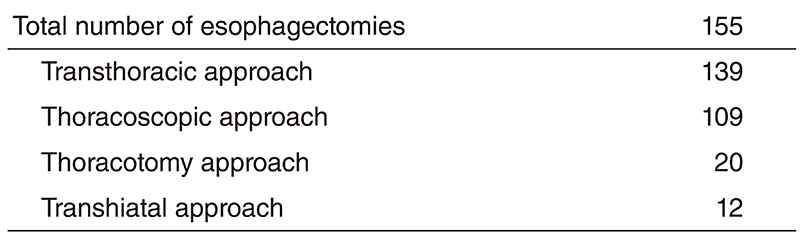
Table 2. Type of Procedures for cervical esophageal cancer

Research activities
To achieve the best practice for patients, we are investigating tissue perfusion imaging studies in several aspects. First, using O2 saturation imaging, we are exploring the best gastric conduit and most suitable anastomotic site during surgery. Second, using AI deep learning technology, we are focusing on AI guide real time surgery particularly focusing on the anatomical recognition recurrent laryngeal nerves to avoid unexpected injuries and subsequent recurrent nerve palsy which greatly impair the patients' quality of life after surgery. Third, regarding the preoperative status of patients and their families, we are doing a case-control trail into whether or not an active preoperative rehabilitation program with a nutrition program would improve the postoperative patient status particularly the skeletal mass index (which is vital to avoid sarcopenia) and reduce postoperative fatigue after surgery. Several other research activities are planned at this point.
Clinical trials
Currently, our department is examining the role of thoracolaparoscopic esophagectomy as a minimally invasive esophagectomy that consists of thoracoscopic esophagectomy and laparoscopic reconstruction. For patients who do not undergo radical chemoradiotherapy, thoracoscopic esophagectomy in the prone position with radical lymph node dissection and laparoscopic reconstruction after esophagectomy for patients without a history of laparotomy are being attempted with the aim of becoming a standard surgical procedure for esophageal cancer. For treating patients aged over 80 or at high risk, a two-stage surgical procedure divided into resection and reconstruction is being attempted.
A randomized controlled phase III study comparing Cisplatin and 5-fluorouracil versus Cisplatin and 5-fluorouracil plus Docetaxel versus Cisplatin and 5-fluorouracil concurrent radiation as a neoadjuvant treatment for locally advanced esophageal cancer is ongoing. A randomized controlled phase III study of minimally invasive versus open esophagectomy for thoracic esophageal cancer (JCOG1409, MONET trial) is also ongoing. Since 2000, our department has started to perform salvage surgery for patients in whom definitive chemoradiotherapy has failed. The operative procedures and postoperative management have been refined gradually. Our department is also studying the role and efficacy of salvage surgery in the multimodal treatment of esophageal cancer.
Education
In academic training, we teach our residents not only about surgical practices but also academic activities for PhD courses. One of our residents acquired their PhD in 2018. And I am teaching two PhD course students in research activities.
Future prospects
We are exploring best clinical practices for patients and their families. To achieve this mission, we are exploring best surgical practices and future research activities in cooperation with other domestic and international research faculties.
Publications
1. Non-occlusive mesenteric ischemia associated with enteral feeding after esophagectomy for esophageal cancer: report of two cases and review of the literature. Kurita D, Fujita T, Horikiri Y, Sato T, Fujiwara H, Daiko H. Surg Case Rep. 2019 Feb 20;5(1):36. doi: 10.1186/s40792-019-0580-2.
2. Internal hernia to the retrosternal space is a rare complication after minimally invasive esophagectomy: three case reports. Sato T, Fujita T, Fujiwara H, Daiko H. Surg Case Rep. 2019 Feb 18;5(1):26. doi: 10.1186/ s40792-019-0578-9.
List of papers published in 2018
Journal
1. Hashimoto J, Kato K, Ito Y, Kojima T, Akimoto T, Daiko H, Hamamoto Y, Matsushita H, Katano S, Hara H, Tanaka Y, Saito Y, Nagashima K, Igaki H. Phase II feasibility study of preoperative concurrent chemoradiotherapy with cisplatin plus 5-fluorouracil and elective lymph node irradiation for clinical stage II/III esophageal squamous cell carcinoma. Int J Clin Oncol, 24:60-67, 2019
2. Sato T, Fujita T, Fujiwara H, Daiko H. Internal hernia to the retrosternal space is a rare complication after minimally invasive esophagectomy: three case reports. Surg Case Rep, 5:26, 2019
3. Fujita T, Sato T, Sato K, Hirano Y, Fujiwara H, Daiko H. Clinical manifestation, risk factors and managements for postoperative chylothorax after thoracic esophagectomy. J Thorac Dis, 11:S198-S201, 2019
4. Wada S, Inoguchi H, Sadahiro R, Matsuoka YJ, Uchitomi Y, Sato T, Shimada K, Yoshimoto S, Daiko H, Shimizu K. Preoperative Anxiety as a Predictor of Delirium in Cancer Patients: A Prospective Observational Cohort Study. World J Surg, 43:134-142, 2019
5. Nishiumi S, Fujigaki S, Kobayashi T, Kojima T, Ito Y, Daiko H, Kato K, Shoji H, Kodama Y, Honda K, Yoshida M. Metabolomics-based Discovery of Serum Biomarkers to Predict the Side-effects of Neoadjuvant Chemoradiotherapy for Esophageal Squamous Cell Carcinoma. Anticancer Res, 39:519-526, 2019
6. Fujigaki S, Nishiumi S, Kobayashi T, Suzuki M, Iemoto T, Kojima T, Ito Y, Daiko H, Kato K, Shouji H, Honda K, Azuma T, Yoshida M. Identification of serum biomarkers of chemoradiosensitivity in esophageal cancer via the targeted metabolomics approach. Biomark Med, 12:827-840, 2018
7. Nozaki I, Mizusawa J, Kato K, Igaki H, Ito Y, Daiko H, Yano M, Udagawa H, Nakagawa S, Takagi M, Kitagawa Y. Impact of laparoscopy on the prevention of pulmonary complications after thoracoscopic esophagectomy using data from JCOG0502: a prospective multicenter study. Surg Endosc, 32:651-659, 2018
8. Koyanagi K, Kato F, Kanamori J, Daiko H, Ozawa S, Tachimori Y. Clinical significance of esophageal invasion length for the prediction of mediastinal lymph node metastasis in Siewert type II adenocarcinoma: A retrospective single-institution study. Ann Gastroenterol Surg, 2:187-196, 2018
9. Komatsu H, Watanuki S, Koyama Y, Iino K, Kurihara M, Uesugi H, Yagasaki K, Daiko H. Nurse Counseling for Physical Activity in Patients Undergoing Esophagectomy. Gastroenterol Nurs, 41:233-239, 2018
10. Kato F, Monma S, Koyanagi K, Kanamori J, Daiko H, Igaki H, Tachimori Y. Long-term outcome after resection for recurrent oesophageal cancer. J Thorac Dis, 10:2691-2699, 2018
11. Okada N, Fujita T, Kanamori J, Sato A, Horikiri Y, Sato T, Fujiwara H, Daiko H. A case report of postoperative VRSA enteritis: Effective management of rifampicin for vancomycin resistant Staphylococcus aureus enteritis after esophagectomy and colon reconstruction. Int J Surg Case Rep, 52:75-78, 2018
12. Fujiwara H, Kanamori J, Nakajima Y, Kawano T, Miura A, Fujita T, Akita K, Daiko H. An anatomical hypothesis: a "concentric-structured model" for the theoretical understanding of the surgical anatomy in the upper mediastinum required for esophagectomy with radical mediastinal lymph node dissection. Dis Esophagus, 2018
13. Tamaoki M, Komatsuzaki R, Komatsu M, Minashi K, Aoyagi K, Nishimura T, Chiwaki F, Hiroki T, Daiko H, Morishita K, Sakai Y, Seno H, Chiba T, Muto M, Yoshida T, Sasaki H. Multiple roles of single-minded 2 in esophageal squamous cell carcinoma and its clinical implications. Cancer Sci, 109:1121-1134, 2018
14. Kadota T, Hatogai K, Yano T, Fujita T, Kojima T, Daiko H, Fujii S. Pathological tumor regression grade of metastatic tumors in lymph node predicts prognosis in esophageal cancer patients. Cancer Sci, 109:2046-2055, 2018
15. Sato T, Fujita T, Okada N, Fujiwara H, Kojima T, Hayashi R, Daiko H. Postoperative pulmonary complications and thoracocentesis associated with early versus late chest tube removal after thoracic esophagectomy with three-field dissection: a propensity score matching analysis. Surg Today, 48:1020-1030, 2018