Annual Report 2018
Department of Gastric Surgery
Takahiro Kinoshita, Masanori Tokunaga, Akio Kaito, Shizuki Sugita, Masahiro Watanabe, Akiko Tonouchi, Yuri Tanaka, Reo Sato, Eigo Akimoto, Takeshi Ono, Akira Kameyama
Introduction
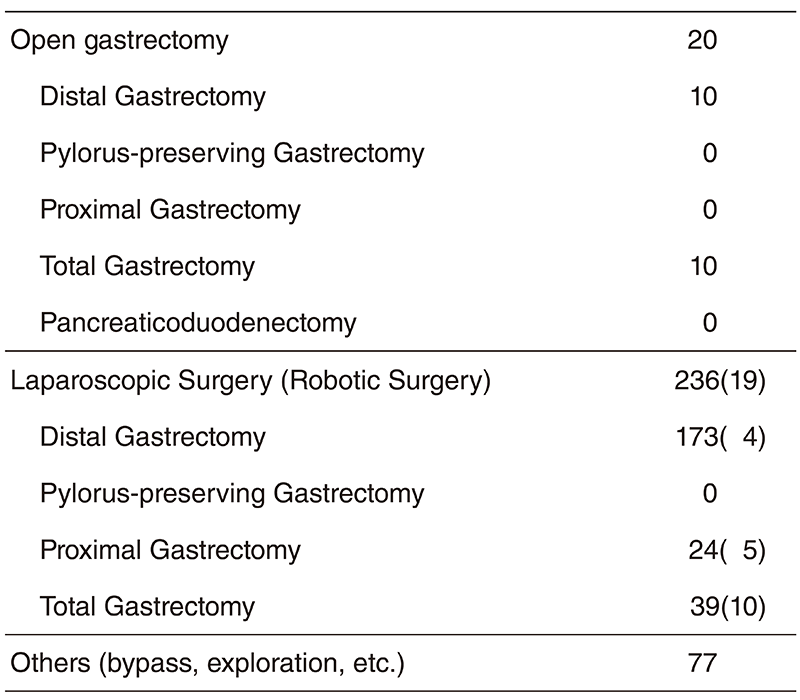
Our Division consists of three staff surgeons, four senior resident and four junior resident surgeons. Our managing of tumors includes common gastric adenocarcinoma, adenocarcinoma of the esophagogastric junction (AEG: Siewert type 2/3), and gastric submucosal tumors (GIST, etc.). Annually, 260-300 patients are operated on either by means of open surgery, laparoscopic or robotic surgery (Table 1). Laparoscopic gastrectomy with radical node dissection was introduced in 2010, and now our department is one of the leading institutions in Japan. In 2018, more than 90% of gastrectomies were performed under laparoscopy or by robot (Table 2). The basis of our surgery is radical extirpation of cancer lesions, but at the same time, organ functions and better quality of life (QOL) should be maintained. In addition, we strive to obtain better clinical outcomes for patients with diseases with dismal prognoses (type 4 gastric cancer or with progressive metastasis) by surgery combined with a modern chemotherapy regimen in cooperation with medical oncologists.

The Team and What We Do
Usually 14-16 patients are hospitalized and six to eight patients undergo operations per week. A clinical conference of our Division is held once a week to decide our treatment strategy. Further, a conference with internal medicine is held every week with doctors of Medical Oncology and Gastrointestinal Endoscopy, discussing the accurate diagnosis of the patients to decide the optimal treatment method. In principle, patients with low-risk superficial gastric cancer lesions (cT1a) are treated by endoscopic submucosal dissection (ESD) following the criteria of the guideline. Some are required to undergo subsequent completion laparoscopic surgery with nodal dissection based on pathological findings of specimens obtained by ESD. Laparoscopic (robot) surgery covers distal, proximal, pyloruspreserving, and total gastrectomy. D2 dissection can also be done, and its indication is expanding to advanced cancer. When the tumor infiltrates to adjacent organs, sometimes extended operations are chosen. Recently, due to the progress of chemotherapy regimen, down-staging from cStageIV is sometimes seen. For such patients, we selectively perform conversion surgery to achieve favorable outcomes. For AEGs, the transhiatal approach can be safely employed under laparoscopy with a better surgical view.
Research activities
We aggressively publish our clinical research data in domestic and international congresses. In addition, we participate in multi-institutional clinical trials conducted by the Japan Clinical
Oncology Group (JCOG) - Gastric Surgery Study Group or other international and domestic organizations. Patients with gastric cancer are, if eligible for each study, invited to take part in one of the ongoing clinical trials.
Clinical trials
The list of clinical trials in which we participated in 2018 is as below.
1) JCOG1301C A randomized phase II study of systemic chemotherapy with and without trastuzumab followed by surgery in HER2 positive advanced gastric or esophagogastric junction adenocarcinoma with extensive lymph node metastasis (Trastuzumab In Gastric or Esophagogastric junction Adenocarcinoma)
2) JCOG1509 Phase III trial to evaluate the efficacy of neoadjuvant chemotherapy with S-1 plus oxaliplatin followed by D2 gastrectomy with adjuvant S-1 in locally advanced gastric cancer (NAGISA trial)
3) A Phase III, Randomized, Double-Blind, Clinical Trial of Pembrolizumab (MK3475) Plus Chemotherapy (XP or FP) Versus Placebo Plus Chemotherapy (XP or FP) as Neoadjuvant/Adjuvant Treatment for Subjects With Gastric and Gastroesophageal Junction (GEJ) Adenocarcinoma (KEYNOTE-585)
4) Extensive Peritoneal Lavage after Curative Gastrectomy for Gastric Cancer: a Randomized Controlled Trial (EXPEL Study)
5) A phase II study of systemic chemotherapy with S-1 and Oxaliplatin followed by gastrectomy with D2 or D2 plus limited paraaortic lymph node dissection in HER2 negative advanced gastric or esophagogastric junction cancer with extensive lymph node metastasis (SOX-D2 study)
6) Venous Thromboembolism (VTE) in Cancer Patients; a Multicenter Prospective Registry
Education
Resident doctors are trained to be specialized surgical oncologists with sufficient techniques and knowledge. Nowadays, opportunities to perform laparoscopic and open surgery are simultaneously given to them. We also place importance on the education of surgeons of other institutions. In 2018, surgeons from domestic and foreign hospitals (from China, Argentina, Colombia, Spain, Slovenia, and Russia) visited our division to learn surgical techniques.
Future prospects
We will keep striving to obtain better survival outcomes for the patients with far advanced diseases; for multidisciplinary therapy (chemotherapy, molecular-target agents or immune check-point inhibitor), collaborating with medical oncologists is essential. Additionally, we will continue to develop less-invasive as well as high-quality surgical methods (laparoscopic or robotic surgery), to improve patients' QOL and realize complete cures. It is also our obligation to expand our knowledge and experience globally as one of the main countries in terms of gastric cancer occurrence.
List of papers published in 2018
Journal
1. Liu H, Kinoshita T, Tonouchi A, Kaito A, Tokunaga M. What are the reasons for a longer operation time in robotic gastrectomy than in laparoscopic gastrectomy for stomach cancer? Surg Endosc, 33:192-198, 2019
2. Oono Y, Kuwata T, Takashima K, Shinmura K, Hori K, Yoda Y, Ikematsu H, Shitara K, Kinoshita T, Yano T. Human epidermal growth factor receptor 2-, epidermal growth factor receptor-, and mesenchymal epithelial transition factor-positive sites of gastric cancer using surgical samples. Gastric Cancer, 22:335-343, 2019
3. Uyama I, Suda K, Nakauchi M, Kinoshita T, Noshiro H, Takiguchi S, Ehara K, Obama K, Kuwabara S, Okabe H, Terashima M. Clinical advantages of robotic gastrectomy for clinical stage I/II gastric cancer: a multi-institutional prospective single-arm study. Gastric Cancer, 22:377-385, 2019
4. Tonouchi A, Kinoshita T, Watanabe M, Sugita S, Kaito A, Tokunaga M. Laparoscopic total gastrectomy for gastric cancer with adult intestinal malrotation: a case report. Dig Med Res [Internet], 1:7, 2018
5. Watanabe M, Kinoshita T, Tokunaga M, Kaito A, Sugita S. Complications and their correlation with prognosis in patients undergoing total gastrectomy with splenectomy for treatment of proximal advanced gastric cancer. Eur J Surg Oncol, 44:1181-1185, 2018
6. Oono Y, Kuwata T, Takashima K, Yoda Y, Ikematsu H, Shitara K, Kinoshita T, Yano T. Clinicopathological features and endoscopic findings of HER2-positive gastric cancer. Surg Endosc, 32:3964- 3971, 2018