Annual Report 2018
Department of Breast Surgery
Takayuki Kinoshita, Shin Takayama, Kenjiro Jimbo, Sho Shiino, Takeshi Murata, Chikashi Watase
Introduction
The Department of Breast Surgery deals with treatment of breast disease through surgeries, as well as diagnosis of breast diseases and assessment of lymph nodes in the axillary and clavicular regions which are suspected of harboring metastases. In fiscal 2018, we performed a total of 894 operations on breast diseases (770 were primary breast cancer or breast sarcoma) (Table 1. Table 2-1). As the "Table" shows, the number of patients we treat is increasing year by year, and the figure for 2018 was the highest ever in our department. Surgical procedure trends have also been changing in recent years. Although breast partial resection (Bp) accounted for 39% of the total surgeries in our department in 2018, the Bp rate has been constant. On the other hand, immediate reconstruction surgeries have rapidly increased in recent years. One of the reasons is the increasing needs of patients for immediate reconstruction surgeries. In our hospital, since 2010, immediate breast reconstruction became one of the choices for patients for whom breast preservation was cosmetically difficult, and a total of 172 immediate breast reconstructions were performed in fiscal 2018 comprising 22% of all cases. One hundred and ten of 172 were tissue expander (TE) operations and 20 direct implant (DIM), and 18 autologous reconstruction (35 DIEP; deep inferior epigastric perforator flap, and seven LD; latissimus dorsi muscle flap) (Table2-2) were performed. We perform these reconstruction surgeries in cooperation with plastic surgeons depending on patients' needs. And the new less invasive technique, radiofrequency abrasion (RFA), is another topic of our surgeries. RFA is a new treatment which boils tumors using electro-radio waves; in addition, it reduces the physical burden on patients and breast deformation after surgery. So as to make RFA one of the standard treatments in breast cancer in the near future, we are currently researching the efficacy and safety of RFA (RAFAELO and PO-RAFAELO study). Although RAFAELO study recruitment ended in 2017, new recruitment for the PO-RAFAELO study started at the end of fiscal 2018. And in fiscal 2018, one RFA was newly performed. In the future, we think that the number of RFA is expected to increase with the registration of this new study. When focusing on axillary staging management, sentinel lymph node (SLN) biopsies (SLNB) were performed in 78% of cases. Following SLNB, the axillary lymph node dissection (ALND) could be avoided when the SLNB was negative. Another new challenge we are engaging in concerns OSNA (One-step nucleic acid amplification). OSNA quantitatively measures CK19 mRNA from sentinel lymph node metastases even at molecular levels. And in conjunction with this assay and conventional microscopic method, we began to be able to evaluate the SLN more precisely. Further, by comparing the OSNA results with that of conventional histological diagnosis, we try to realize the possibility of omitting axillary lymph node dissection by using two methods. As a result, we established a model for intraoperatively predicting axillary lymph node metastasis based on the combined use of OSNA and histological examination (NCS score), and these results were published in the European Journal of Surgical Oncology (Nov 2019). We believed that axillary dissection can be omitted for clinical node negative patients by using this prediction model, and we thought that the use of this model will facilitate the selection of optimal adjuvant therapies without requiring unnecessary axillary lymph node dissection. Thus, we are striving continuously to meet the diverse needs of breast cancer patients.
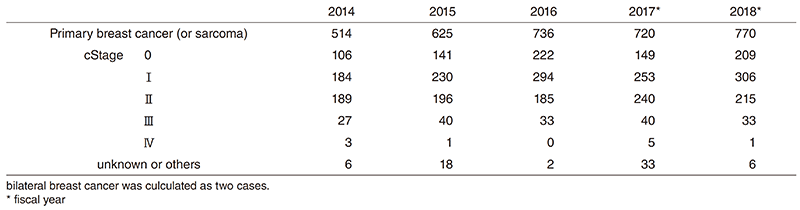
Table 2-1. Type of procedure (breast surgery)
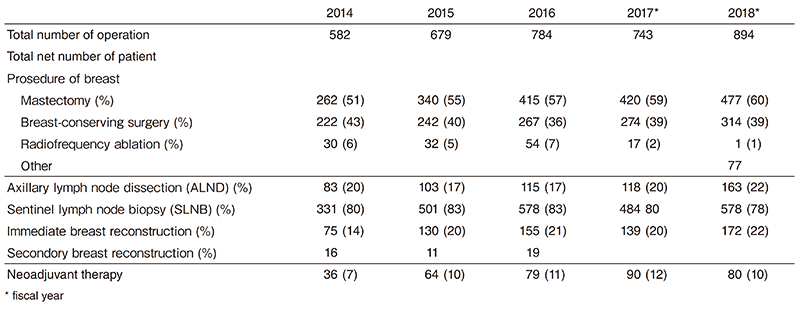
Table 2-2. Type of procedure (reconstruction surgery)

The Team and What We Do
Our department is comprised of five staff surgeons specialized in breast cancer (Dr. Kinoshita, Dr. Takayama, Dr. Jimbo, Dr. Shiino, and Dr. Murata), one chief resident (Dr. Watase), and two or three rotating residents. From 7:15 every morning, all the staff and residents perform in-patient rounds together. Journal clubs and research conferences are scheduled for every Tuesday morning after rounds. Weekly conferences are held on Monday from 17:30 to 19:00, and on Wednesday from 17:00 to 18:00 for shared discussions with surgeons, and the diagnostic images of pre-operative patients are reviewed and compared with pathological reports in every postoperative patient. A breast pathology/imaging conference is held on the second Wednesday every two months from 19:00 to 20:00 to discuss problems with diagnostic imaging, and with pathologically interesting cases. A conference about studies, institutional treatment guidelines, and recent topics regarding breast cancer is also held irregularly by a multidisciplinary team. Treatment Guidelines for primary and metastatic breast cancer have been updated regularly through this multidisciplinary discussion since 2003.
Surgery
We perform surgeries from Monday to Friday; there are usually 15 to 18 cases of breast cancer in a week. Table 1 shows the total number of patients with primary breast cancer (including breast primary sarcoma) and other breast diseases. The types and number of operative procedures are shown in Table 2. The rate of mastectomy was 477 cases (60%), including 172 cases of immediate reconstruction. SLNB was performed on 578 (78%) patients, and many patients were spared from ALND in 2018.
Research activities and Clinical trials
1. Radiofrequency ablation therapy for early breast cancer as local therapy (RAFAELO study)
2. Patients offered Radio Radiofrequency ablation therapy for early breast cancer as local therapy (PO-RAFAELO study)
3. Intensive versus standard post-operative surveillance in high risk breast cancer patients (JCOG1204, INSPIRE Trial)
4. Single-arm confirmatory trial of endocrine therapy alone for estrogen positive, low-risk ductal carcinoma in situ of the breast (Low-risk DCIS with endocrine therapy alone-TAM) (JCOG1505, LORETTA Trial)
5. Postoperative Therapy with Endocrine and TS-1 (POTENT study)
6. Registration Data-base System of breast cancer patients who received lymph node metastasis diagnosis by the OSNA method (LynoLog Data-base)
7. Olaparib as Adjuvant Treatment in Patients With Germline BRCA Mutated High Risk HER2 Negative Primary Breast Cancer (OlympiA)
8. Hair Loss Prevention System with chemotherapy-induced alopecia in breast cancer patients in Japan (HOPE)
Future prospects
The aims of our activities are as follows:
1. Clinical activities
To provide the very best breast surgical treatment
2. Research activities
To develop less invasive breast surgical procedures
3. Educational activities
To train specialists in breast cancer who lead the future of cancer fields.
List of papers published in 2018
Journal
1. Tsuchiya M, Masujima M, Kato T, Ikeda SI, Shimizu C, Kinoshita T, Shiino S, Suzuki M, Mori M, Takahashi M. Knowledge, fatigue, and cognitive factors as predictors of lymphoedema risk-reduction behaviours in women with cancer. Support Care Cancer, 27:547-555, 2019
2. Hironaka-Mitsuhashi A, Tsuda H, Yoshida M, Shimizu C, Asaga S, Hojo T, Tamura K, Kinoshita T, Ushijima T, Hiraoka N, Fujiwara Y. Invasive breast cancers in adolescent and young adult women show more aggressive immunohistochemical and clinical features than those in women aged 40-44 years. Breast Cancer, 26:386-396, 2019
3. Shiino S, Matsuzaki J, Shimomura A, Kawauchi J, Takizawa S, Sakamoto H, Aoki Y, Yoshida M, Tamura K, Kato K, Kinoshita T, Kitagawa Y, Ochiya T. Serum miRNA-based Prediction of Axillary Lymph Node Metastasis in Breast Cancer. Clin Cancer Res, 25:1817-1827, 2019
4. Asaga S, Kinoshita T, Shiino S, Jimbo K, Takayama S. Prognostic factors for breast cancer patients with T1-2 tumor and 1-3 positive axillary nodes treated using total mastectomy without radiotherapy. Breast J, 25:26-33, 2019
5. Kinoshita T. RFA experiences, indications and clinical outcomes. Int J Clin Oncol, 24:603-607, 2019
6. Shiino S, Yoshida M, Jimbo K, Asaga S, Takayama S, Maeshima A, Tsuda H, Kinoshita T, Hiraoka N. Two rare cases of endosalpingiosis in the axillary sentinel lymph nodes: evaluation of immunohistochemical staining and one-step nucleic acid amplification (OSNA) assay in patients with breast cancer. Virchows Arch, 474:633-638, 2019
7. Kitajima K, Nakatani K, Yamaguchi K, Nakajo M, Tani A, Ishibashi M, Hosoya K, Morita T, Kinoshita T, Kaida H, Miyoshi Y. Response to neoadjuvant chemotherapy for breast cancer judged by PERCIST - multicenter study in Japan. Eur J Nucl Med Mol Imaging, 45:1661-1671, 2018
8. Tsuchiya M, Masujima M, Mori M, Takahashi M, Kato T, Ikeda SI, Shimizu C, Kinoshita T, Shiino S, Suzuki M. Information-seeking, information sources and ongoing support needs after discharge to prevent cancer-related lymphoedema. Jpn J Clin Oncol, 48:974-981, 2018
9. Okubo R, Noguchi H, Hamazaki K, Sekiguchi M, Kinoshita T, Katsumata N, Narisawa T, Uezono Y, Xiao J, Matsuoka YJ. Association between blood polyunsaturated fatty acid levels and depressive symptoms in breast cancer survivors. Prostaglandins Leukot Essent Fatty Acids, 139:9-13, 2018
10. Shimoi T, Hamada A, Yamagishi M, Hirai M, Yoshida M, Nishikawa T, Sudo K, Shimomura A, Noguchi E, Yunokawa M, Yonemori K, Shimizu C, Kinoshita T, Fukuda T, Fujiwara Y, Tamura K. PIK3CA mutation profiling in patients with breast cancer, using a highly sensitive detection system. Cancer Sci, 109:2558-2566, 2018
11. Shimoi T, Yoshida M, Kitamura Y, Yoshino T, Kawachi A, Shimomura A, Noguchi E, Yunokawa M, Yonemori K, Shimizu C, Kinoshita T, Ichimura K, Fukuda T, Fujiwara Y, Tamura K. TERT promoter hotspot mutations in breast cancer. Breast Cancer, 25:292-296, 2018
12. Shimazu K, Sato N, Ogiya A, Sota Y, Yotsumoto D, Ishikawa T, Nakamura S, Kinoshita T, Tsuda H, Ohi Y, Akiyama F, Noguchi S. Intraoperative Nomograms, Based on One-Step Nucleic Acid Amplification, for Prediction of Non-sentinel Node Metastasis and Four or More Axillary Node Metastases in Breast Cancer Patients with Sentinel Node Metastasis. Ann Surg Oncol, 25:2603- 2611, 2018
13. Makise N, Sekimizu M, Kubo T, Wakai S, Watanabe SI, Kato T, Kinoshita T, Hiraoka N, Fukayama M, Kawai A, Ichikawa H, Yoshida A. Extraskeletal osteosarcoma: MDM2 and H3K27me3 analysis of 19 cases suggest disease heterogeneity. Histopathology, 73:147-156, 2018