Annual Report 2018
Department of Thoracic Surgery
Shun-ichi Watanabe, Kazuo Nakagawa, Yukihiro Yoshida, Masaya Yotsukura, Yu Okubo
Introduction
The Department of Thoracic Surgery deals with various kinds of neoplasms and allied diseases in the thorax, except the esophagus. These include both primary and metastatic lung tumors, mediastinal tumors, pleural tumors (mesotheliomas) and chest wall tumors. The main clinical activity of our department and the subject of most of its research activities has been the surgical management of lung cancer patients. As well as continuing to improve procedures, such as the combined resection of neighboring vital structures and minimally invasive techniques (video-assisted thoracic surgery, VATS), it has become increasingly important to define the role of surgery in multimodality treatment for patients with poor prognoses.
The Team and What We Do
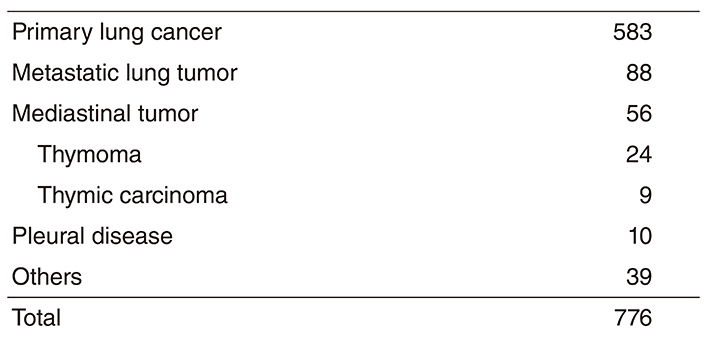
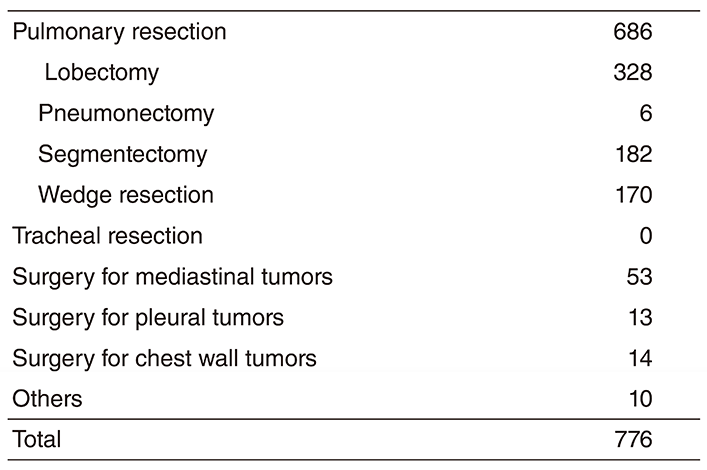
Our department has four attending surgeons and attending and resident surgeons perform all of the inpatient care, operations, examinations and outpatient care. In 2018, we performed a total of 776 operations; for lung cancer in 583 patients, metastatic tumors in 88, mediastinal tumors in 56 and others in 49 (Tables 1 and 2).
The treatment strategy for patients with lung cancer is based on tumor histology (non-small cell vs. small cell), the extent (clinical stage) of the disease (clinical stage) and the physical status of the patient. In lung cancer patients, surgical resection is usually indicated for clinical stages I, II and some IIIA with non-small cell histology and clinical stages I with small cell histology. However, to improve the poor prognosis of patients with clinically and histologically proven mediastinal lymph node metastasis or with invasion of vital neighboring structures, optimal treatment modalities are sought in a clinical trial setting. Recently, adjuvant chemotherapy has often been given to patients with advanced lung cancer, even after complete pulmonary resection.
For metastatic lung tumors, resection has been attempted on the basis of Thomford's criteria: eligible patients are those who are at good risk, with no extrathoracic disease, with the primary site under control and with completely resectable lung disease. Metastasis from colorectal carcinomas is the most common disease.
For mediastinal tumors, thymic epithelial tumors are most commonly encountered for resection. In the mediastinum meanwhile, where various tumor histologies can arise, treatment must be carefully determined by cytologic/ histologic diagnosis before surgery. For patients with thymoma, we have already adopted videoassisted resection (VATS) of the tumor. VATS resection of mediastinal tumor is indicated exclusively for small thymomas.
As for meetings, there are two department meetings. One is for the preoperative evaluation and postoperative inpatient review on Friday and the other is for the journal club on Tuesday. In addition, on Thursday, the chest group holds a plenary meeting to share basic information about current issues for diagnosing and treating patients with lung malignancy.
Research activities
Lymph node dissection for lung cancer has been a major issue in lung cancer treatment and has been extensively studied in our department. We continue to improve our surgical dissection technique taking oncological and surgical aspects into consideration: a more effective and less invasive lymph node dissection called "selective mediastinal/hilar dissection" according to the location of the primary tumor by the lobe.
Minimally invasive open surgery (MIOS), with a thoracoscope for thoracic malignancies, is also an important challenge in our department. Indications and surgical techniques of videoassisted surgery for early lung cancer are of special interest given the increased incidence of such minute tumors due to improvements in CT devices and CT screening.
Clinical trials
The advent of new technologies in CT scanning means more small-sized lung cancers are being found in screening settings and by chance. They are usually present as "groundglass opacity (GGO)" on CT and considered as early adenocarcinoma in pathological terms. The surgical management of such GGO-type lung cancer remains undetermined in terms of the extent of pulmonary parenchymal resection and lymph node dissection. Some cases might be followed up with careful monitoring by CT, since indolent tumors are known to exist and we are seeking how best to manage such patients. A clinical trial to determine the appropriateness of limited resection for early adenocarcinoma had been planned in the Japan Clinical Oncology Group (JCOG) - Lung Cancer Surgical Study Group and two clinical trials (phase III, JCOG 0802 and phase II, JCOG 0804) have been conducted since the end of 2009. In addition, another phase II trial (JCOG 1211), a confirmatory trial of segmentectomy for clinical T1N0 lung cancer dominant with GGO, was started in 2013. The accrual of these three trials having investigated the appropriateness of limited resection is complete and has achieved the planned number of patients. We now await maturation of the follow-up data regarding recurrence and prognosis.
As for lymph node dissection, a randomized phase III trial of lobe-specific versus systematic nodal dissection for c-stage I/II nonsmall cell lung cancer (JCOG 1413) opened to accrual in January 2017, as did sublobar resection versus lobectomy for patients with resectable stage I non-small cell lung cancer with idiopathic pulmonary fibrosis in a phase III study evaluating survival (JCOG1708) in May 2018. More recently, prospective observational study of daily living activities in elderly patients having undergone lung cancer surgery (JCOG1710A) opened to accrual.
As for postoperative adjuvant therapy, a phase III clinical trial to compare the effectiveness of UFT with that of TS-1 for stage IA exceeding 2 cm and IB NSCLC planned in JCOG (JCOG 0707) has been conducted since 2008. This trial completed the full accrual of 960 patients in 2013. A phase III clinical trial (JCOG 1205) to compare Irinotecan/Cisplatin with Etoposide/ Cisplatin for adjuvant chemotherapy of resected pulmonary high-grade neuroendocrine carcinoma was started in 2013. This trial also completed the full accrual of 221 patients in 2018. We are await the maturation of follow-up data regarding recurrence and prognosis.
List of papers published in 2018
Journal
1. Makise N, Sekimizu M, Konishi E, Motoi T, Kubo T, Ikoma H, Watanabe SI, Okuma T, Hiraoka N, Fukayama M, Kawai A, Ichikawa H, Yoshida A. H3K27me3 deficiency defines a subset of dedifferentiated chondrosarcomas with characteristic clinicopathological features. Mod Pathol, 32:435-445, 2019
2. Okami J, Shintani Y, Okumura M, Ito H, Ohtsuka T, Toyooka S, Mori T, Watanabe SI, Date H, Yokoi K, Asamura H, Nagayasu T, Miyaoka E, Yoshino I. Demographics, Safety and Quality, and Prognostic Information in Both the Seventh and Eighth Editions of the TNM Classification in 18,973 Surgical Cases of the Japanese Joint Committee of Lung Cancer Registry Database in 2010. J Thorac Oncol, 14:212-222, 2019
3. Uchida S, Watanabe SI, Yoshida Y, Kobayashi A, Asakura K, Nakagawa K. Aberrant mediastinal trunk of pulmonary artery. J Surg Case Rep, 2019:rjy359, 2019
4. Uchida S, Tsuta K, Kusumoto M, Shiraishi K, Kohno T, Watanabe SI. Radiopathologic correlation of collision lung cancer with ground-glass opacity. Asian Cardiovasc Thorac Ann, 27:45-48, 2019
5. Yoshida Y, Sakane T, Isogai J, Suzuki Y, Miki S, Nomura Y, Nakajima J. Computer-assisted detection of metastatic lung tumors on computed tomography. Asian Cardiovasc Thorac Ann, 27:199- 207, 2019
6. Yoshida Y, Manaka T, Nitadori JI, Shinozaki-Ushiku A, Doke T, Saito T, Sato J, Miyaji T, Yamaguchi T, Oyama H, Fukayama M, Nakajima Y, Nakajima J. A comparison between 2- and 3-dimensional approaches to solid component measurement as radiological criteria for sublobar resection in lung adenocarcinoma ≤ 2 cm in size. Surg Today, 2019
7. Toyoshima Y, Hara T, Matsui Y, Nagumo Y, Maejima A, Shinoda Y, Komiyama M, Watanabe SI, Fujimoto H. Nodule Size After Chemotherapy and Primary-Tumor Teratoma Components Predict Malignancy of Residual Pulmonary Nodules in Metastatic Nonseminomatous Germ Cell Tumor. Ann Surg Oncol, 25:3668- 3675, 2018
8. Makise N, Sekimizu M, Kubo T, Wakai S, Watanabe SI, Kato T, Kinoshita T, Hiraoka N, Fukayama M, Kawai A, Ichikawa H, Yoshida A. Extraskeletal osteosarcoma: MDM2 and H3K27me3 analysis of 19 cases suggest disease heterogeneity. Histopathology, 73:147-156, 2018
9. Giroux DJ, Van Schil P, Asamura H, Rami-Porta R, Chansky K, Crowley JJ, Rusch VW, Kernstine K. The IASLC Lung Cancer Staging Project: A Renewed Call to Participation. J Thorac Oncol, 13:801-809, 2018
10. Suzuki S, Sakurai H, Yotsukura M, Masai K, Asakura K, Nakagawa K, Motoi N, Watanabe SI. Clinical Features of Ground Glass Opacity-Dominant Lung Cancer Exceeding 30 cm in the Whole Tumor Size. Ann Thorac Surg, 105:1499-1506, 2018
11. Miura A, Mori T, Yoshida A, Watanabe Y, Sunami K, Watanabe S, Kohno T, Tsuta K. Primary adenocarcinoma of the trachea revealing a mucinous bronchial gland cell origin. Pathol Res Pract, 214:796-799, 2018
12. Nakagawa K. Validation of the latest WHO histological classification and the 8th TNM staging system for thymic epithelial tumors. Mediastinum, 2:14, 2018