Annual Report 2018
Cancer Screening Center
Takahisa Matsuda, Masau Sekiguchi, Keiko Nakamura, Yasuo Kakugawa, Minori Matsumoto, Masayoshi Yamada, Hiroyuki Takamaru, Takaaki Tsuchida, Masahiko Kusumoto, Gen Iinuma, Nachiko Uchiyama, Mari Kikuchi, Kimiteru Ito, Takahiro Morita, Hiroaki Kurihara, Miyuki Sone, Yasunori Mizuguchi, Hirokazu Watanabe, Mototaka Miyake, Syunsuke Sugawara, Yuko Kubo, Chihiro Ito, Nao Kikkawa, Yasuyuki Ohnishi, Shintaro Kimura, Shinji Fujizuka, Haruto Sugawara, Sawako Kaku, Tomoyasu Kato, Mitsuya Ishikawa, Masaya Uno, Yasuhito Tanase, Takashi Uehara, Mayumi Kato, Hanako Shimizu, Kenichi Nakamura, Hiroshi Takayama, Junko Eba, (Visiting Researcher) Ryutaro Kakinuma, Koichi Nagata, Shogo Endo, Kazutomo Togashi, Noriaki Takahashi, Takaaki Yasuda, Masaki Matsuoka, Ken Takabayashi, Hidenori Kanazawa, Shuji Yamamoto, Hidetsugu Yamagishi, Kayoko Kasuya, (Special research assistant) Mika Mori, Hiroko Shindo
Introduction
In the Cancer Screening Center (former name: Research Center for Cancer Prevention and Screening; RCCPS), we have provided opportunistic cancer screening by using newly developed modalities since 2004. Most of the staff doctors hold two positions concurrently in both the Cancer Screening Center and their own specialized department. Our Cancer Screening Center consists of 18 radiologists, seven gastroenterologists, one bronchoscopist, five gynecologists, seven radiologic technologists, five ultrasonographic technologists and four nurses. Our division is in charge of multiphasic cancer screening using several imaging modalities to develop new cancer screening systems and to assess new screening tests. All medical images are digitalized and all imaging diagnosis can be made from CRT monitors.
The Team and What We Do
1. Course of cancer screening
The basic plan for males consists of screening for cancer of the lung, esophagus, stomach, colorectum, liver, gall bladder, pancreas, kidney, and prostate. In the basic plan for females, the screening for cancer of the breast, uterus, and ovary are added to the plan for males, excluding the prostate. In addition, PET (positron emission tomography) is provided as an option. Other than multiphasic programs, an independent cancer screening program has been prepared for lung and female genital cancers, including cancer of the uterus and ovary, breast cancer and gastrointestinal cancer. Blood samples are also obtained for biochemistry and tumor markers such as CA19-9, CEA, CA125, PSA, and genetic analysis.
2. Eligibility criteria for participants
The cancer screening program at the Cancer Screening Center from 2013 has been planned for applicants 40 years or older who give written informed consent for the screening, including blood samples for genetic analysis, and who take the questionnaire survey concerning lifestyles. These study protocols have been approved by the Institutional Review Board (IRB). Applicants who have been diagnosed as having cancer, and/or have a history of cancer treatment, such as surgery or endoscopic mucosal resection or chemotherapy within the previous one year, are excluded.
3. Cancer screening methods
In the multiphasic cancer screening programs (comprehensive cancer screening program), CT for lung cancer, abdominal US for cancer of the liver, gall bladder, pancreas, and kidney, gynecological examinations with pap-smear and HPV test for uterus cancer, and MMG/ Tomosynthesis and US for breast cancer are performed on the first day. On the following day, gastroscopy for cancer of the esophagus and stomach, and total colonoscopy for cancer of the colon and rectum are conducted. Moreover, from the beginning of December 2010, CTcolonography (CTC) has been provided as an optional method for cancer screening. FDG-PET/ CT is offered on the first day as an option, if the participants wish to undergo the examination. Furthermore, FDG-PET/MRI has been provided as an optional examination since 2018.
4. Number of participants of cancer screening
We present the number of participants of cancer screening between April 2018 and March 2019 in this report (Tables 1, 2). A total of 2,910 people received cancer screening at the Cancer Screening Center in this period. Most of the participants (81%; n=2,359) chose the comprehensive cancer screening course. Regarding the cancer detection rate data in each modality, we will report them in the near future.
Table 1. Number of participants in "Comprehensive cancer screening program"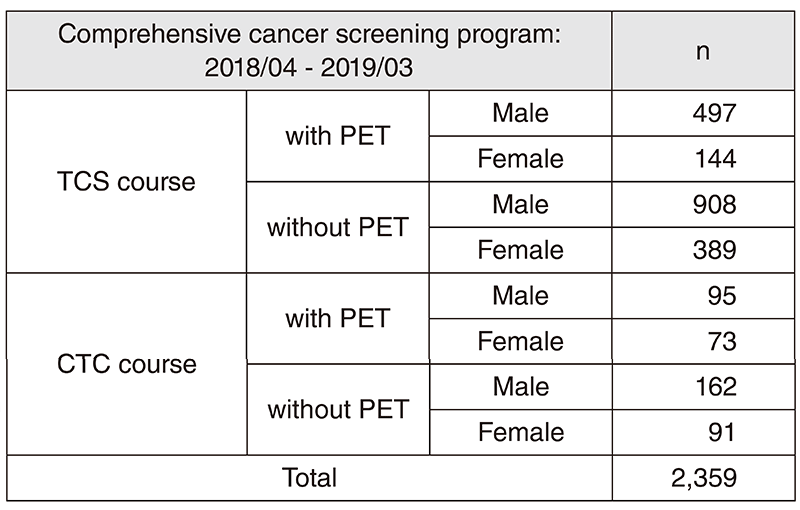
Table 2. Number of participants in "Independent cancer screening course" 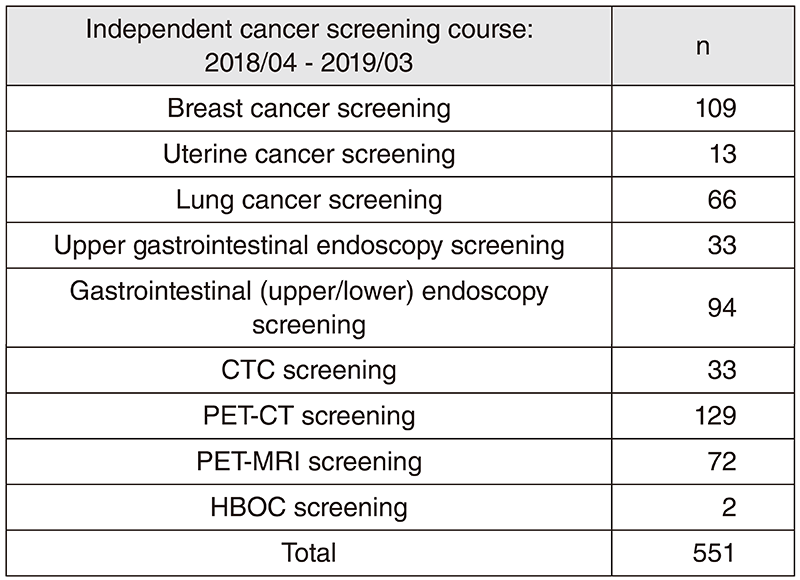
Research activities(Main achievements)
1) Gastric cancer detection rate by upper gastrointestinal endoscopy (EGD) screening: We retrospectively examined the data of the first screening examinees who performed upper gastrointestinal endoscopy (EGD) screening at our center. Of 15,161 subjects (male/female: 9,165/5,996, average age: 63 years old, endoscopic atrophic gastritis prevalence: 59%), 126 cases (0.83%) of gastric cancer detected, of which 115 cases were early advanced gastric cancer: 11 cases.
2) Risk stratification of advanced colorectal neoplasia using background factors: Based on data of individuals undergoing initial colonoscopy at our screening center from February 2004 to March 2013, age, gender, family history of colorectal cancer, smoking status, advanced neoplasia's risk stratification using BMI A scoring score was created and a paper was published (Sekiguchi M, et al. J Gastroenterol. 2018). In the future, we will verify the cost-effectiveness of the validation test and colorectal cancer screening using risk stratification.
3) Observational study of lung cancer CT screening: The characteristics of lung cancer in smokers and non-smokers were evaluated for those who had undergone lung cancer CT screening at this center between February 2004 and March 2012. The subjects were 12,114 [non-smokers, 6,021 (49.7%), 4,820 women (39.8%)]. 152 lung cancers were detected in 133 patients. The initial detection rate and cumulative detection rate of lung cancer patients were 1.0% and 1.1%, respectively.
Clinical trials
In our division, we are ongoing research work based on the study protocol titled "Evaluation of effectiveness of cancer screening modality at National Cancer Center". The target modalities are as follows:
1) Upper gastrointestinal endoscopy, 2) Lower gastrointestinal endoscopy, 3) CT colonography, 4) Chest computed tomography (CT), 5) Sputum cytology, 6) Mammography, 7) Breast ultrasonography, 8) FDG-positron emission tomography (PET), 9) Abdomina
Future prospects
Based on cancer screening data such as examination results, medical institution findings, follow-up findings, the questionnaire survey concerning lifestyles for ten years, we commenced assessing them supported by the National Cancer Center Research and Development Fund.
List of papers published in 2018
Journal
1. Wong JCT, Chiu HM, Kim HS, Byeon JS, Matsuda T, Kobayashi N, Wu DC, Ong DE, Sung JJY. Adenoma detection rates in colonoscopies for positive fecal immunochemical tests versus direct screening colonoscopies. Gastrointest Endosc, 89:607-613.e1, 2019
2. Takeuchi Y, Sawaya M, Oka S, Tamai N, Kawamura T, Uraoka T, Ikematsu H, Moriyama T, Arao M, Ishikawa H, Ito Y, Matsuda T. Efficacy of autofluorescence imaging for flat neoplasm detection: a multicenter randomized controlled trial (A-FLAT trial). Gastrointest Endosc, 89:460-469, 2019
3. Sung JJY, Chiu HM, Jung KW, Jun JK, Sekiguchi M, Matsuda T, Kyaw MH. Increasing Trend in Young-Onset Colorectal Cancer in Asia: More Cancers in Men and More Rectal Cancers. Am J Gastroenterol, 114:322-329, 2019
4. Sekiguchi M, Igarashi A, Sakamoto T, Saito Y, Esaki M, Matsuda T. Cost-effectiveness analysis of postpolypectomy colonoscopy surveillance using Japanese data. Dig Endosc, 31:40-50, 2019
5. Yachida T, Oda I, Abe S, Sekiguchi M, Nonaka S, Suzuki H, Yoshinaga S, Taniguchi H, Sekine S, Masugata H, Masaki T, Daiko H, Saito Y. Risk of Lymph Node Metastasis in Patients with the Superficial Spreading Type of Esophageal Squamous Cell Carcinoma. Digestion, 1-6, 2019
6. Inoki K, Kakugawa Y, Takamaru H, Sekiguchi M, Matsumoto M, Matsuda T, Ito A, Tanaka T, Inamoto Y, Fuji S, Kurosawa S, Kim SW, Fukuda T, Ohe Y, Saito Y. Capsule Endoscopy after Hematopoietic Stem Cell Transplantation Can Predict Transplant-Related Mortality. Digestion, 1-10, 2019
7. Kodashima S, Tanaka K, Matsuda K, Fujishiro M, Saito Y, Ohtsuka K, Oda I, Katada C, Kato M, Kida M, Kobayashi K, Hoteya S, Horimatsu T, Matsuda T, Muto M, Yamamoto H, Ryozawa S, Iwakiri R, Kutsumi H, Miyata H, Kato M, Haruma K, Fujimoto K, Uemura N, Kaminishi M, Tajiri H. First progress report on the Japan Endoscopy Database project. Dig Endosc, 30:20-28, 2018
8. Bogie RMM, Veldman MHJ, Snijders LARS, Winkens B, Kaltenbach T, Masclee AAM, Matsuda T, Rondagh EJA, Soetikno R, Tanaka S, Chiu HM, Sanduleanu-Dascalescu S. Endoscopic subtypes of colorectal laterally spreading tumors (LSTs) and the risk of submucosal invasion: a meta-analysis. Endoscopy, 50:263-282, 2018
9. Sakamoto T, Saito Y, Nakamura F, Abe S, Takamaru H, Sekiguchi M, Yamada M, Nakajima T, Matsuda T, Yamagishi H, Kato H. Short-term outcomes following endoscopic submucosal dissection of large protruding colorectal neoplasms. Endoscopy, 50:606-612, 2018
10. Matsuda K, Tanaka K, Fujishiro M, Saito Y, Ohtsuka K, Oda I, Katada C, Kato M, Kida M, Kobayashi K, Hoteya S, Horimatsu T, Kodashima S, Matsuda T, Muto M, Yamamoto H, Ryozawa S, Iwakiri R, Kutsumi H, Miyata H, Kato M, Haruma K, Fujimoto K, Uemura N, Kaminishi M, Tajiri H. Design paper: Japan Endoscopy Database (JED): A prospective, large database project related to gastroenterological endoscopy in Japan. Dig Endosc, 30:5-19, 2018
11. Rutter MD, Beintaris I, Valori R, Chiu HM, Corley DA, Cuatrecasas M, Dekker E, Forsberg A, Gore-Booth J, Haug U, Kaminski MF, Matsuda T, Meijer GA, Morris E, Plumb AA, Rabeneck L, Robertson DJ, Schoen RE, Singh H, Tinmouth J, Young GP, Sanduleanu S. World Endoscopy Organization Consensus Statements on Post-Colonoscopy and Post-Imaging Colorectal Cancer. Gastroenterology, 155:909-925.e3, 2018
12. Sekiguchi M, Kakugawa Y, Matsumoto M, Matsuda T. A scoring model for predicting advanced colorectal neoplasia in a screened population of asymptomatic Japanese individuals. J Gastroenterol, 53:1109-1119, 2018
13. Sakamoto T, Nakajima T, Matsuda T, Murakami Y, Ishikawa H, Yao K, Saito Y. Comparison of the diagnostic performance between magnifying chromoendoscopy and magnifying narrow-band imaging for superficial colorectal neoplasms: an online survey. Gastrointest Endosc, 87:1318-1323, 2018
14. Abe S, Oda I, Minagawa T, Sekiguchi M, Nonaka S, Suzuki H, Yoshinaga S, Bhatt A, Saito Y. Metachronous Gastric Cancer Following Curative Endoscopic Resection of Early Gastric Cancer. Clinical endoscopy, 51:253-259, 2018
15. Abe S, Saito Y, Oono Y, Tanaka Y, Sakamoto T, Yamada M, Nakajima T, Matsuda T, Ikematsu H, Yano T, Sekine S, Kojima M, Yamagishi H, Kato H. Pilot study on probe-based confocal laser endomicroscopy for colorectal neoplasms: an initial experience in Japan. Int J Colorectal Dis, 33:1071-1078, 2018
16. Iwatate M, Sano Y, Tanaka S, Kudo SE, Saito S, Matsuda T, Wada Y, Fujii T, Ikematsu H, Uraoka T, Kobayashi N, Nakamura H, Hotta K, Horimatsu T, Sakamoto N, Fu KI, Tsuruta O, Kawano H, Kashida H, Takeuchi Y, Machida H, Kusaka T, Yoshida N, Hirata I, Terai T, Yamano HO, Nakajima T, Sakamoto T, Yamaguchi Y, Tamai N, Nakano N, Hayashi N, Oka S, Ishikawa H, Murakami Y, Yoshida S, Saito Y. Validation study for development of the Japan NBI Expert Team classification of colorectal lesions. Dig Endosc, 30:642-651, 2018
17. Kudo T, Saito Y, Ikematsu H, Hotta K, Takeuchi Y, Shimatani M, Kawakami K, Tamai N, Mori Y, Maeda Y, Yamada M, Sakamoto T, Matsuda T, Imai K, Ito S, Hamada K, Fukata N, Inoue T, Tajiri H, Yoshimura K, Ishikawa H, Kudo SE. New-generation full-spectrum endoscopy versus standard forward-viewing colonoscopy: a multicenter, randomized, tandem colonoscopy trial (J-FUSE Study). Gastrointest Endosc, 88:854-864, 2018